Background: Many prostate cancers (PCa) have an indolent course that never requires treatment. Prostate biopsy is also not harmless and thus should be avoided if possible. This study aimed to determine if having both a PSA Density (PSAD) < 0.15 ng/mL2 and no GG1 cores from targeted lesions can identify patients on active surveillance (AS) who do not progress to either GG2+ disease or to treatment.
Methods: A prospectively collected cohort of AS patients with MRI-US fusion biopsy and current or previous biopsy documenting maximum GG1 PCa received annual biopsies. The core samples from the targeted lesions were a combination of cores from the targeted biopsy as well as cores from the systematic biopsy that neighbor and overlap the lesion, as determined by the fusion biopsy software. High progression risk was defined as a patient either having a PSAD > 0.15 or at least one GG1 core from a targeted lesion. Sensitivity, specificity, NPV, PPV, regression analysis, and Kaplan-Meier estimates were calculated for the presence of progression to GG2+ disease or treatment within 4 years.
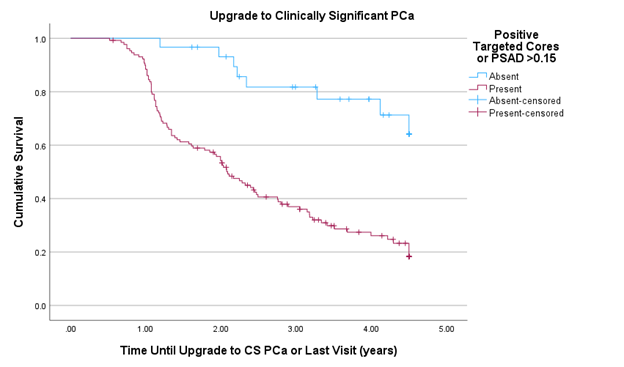
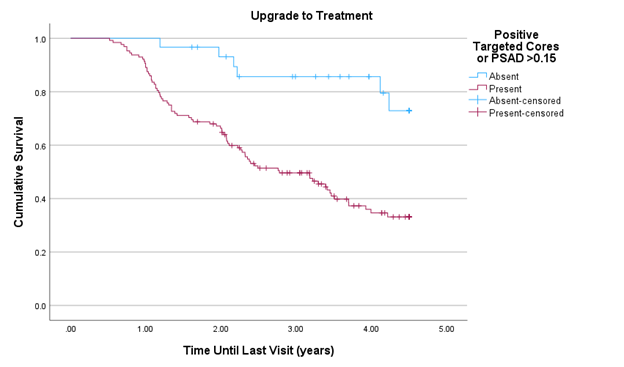
Results: One hundred sixty patients met inclusion criteria. Of these, 141 (88%) patients were GG1 and 19 (12%) were benign on initial MRI-US fusion biopsy. After 4 years, 102 (64%) had progressed to GG2+ and 83 (52%) had undergone treatment for PCa. 130 (81%) had high progression risk, which was associated with a sensitivity of 92.16% and 92.77%, a specificity of 37.93% and 32.00%, a PPV of 72.31% and 60.16%, a NPV of 73.33% and 80.00%, and an odds ratio of 7.18 (p<.001) and 6.04 (p<.001) for progression to GG2+ disease and treatment within 4 years, respectively. When controlling for the number of non-targeted cores and PI-RADS score, progression to GG2+ was not significant (p=0.45), but progression to treatment was (OR 2.61; p=0.03). The high progression risk group had an estimated mean time to progression to GG2+ of 2.49 years (SD 1.45) and to treatment of 2.85 years (SD 1.47). The men with PSAD <0.15 and non-targeted biopsy positivity had an estimated mean time to progression to GG2+ of 3.97 years (SD 1.11) and to treatment of 4.09 years (SD 0.94). If no more biopsies were taken in the lower risk group for the next 4 years, only 8 patients (26.7%) would have missed GG2+ disease and 6 (20%) would have missed receiving treatment.
Conclusion: Having both a PSAD <0.15 ng/mL2 and no positive cores from a targeted lesion on initial MR-US fusion biopsy has both a low risk of progression to GG2+ disease and a low risk of progression to treatment within 4 years of biopsy. This can be used to avoid or delay biopsies in these lower risk AS patients.