Background:Effective communication between pathologists and clinicians is essential for providing safe and appropriate cancer care. Synoptic reporting aims to facilitate communication by creating concise reports that are easy for pathologists to generate, straightforward for clinicians to understand, and accessible for research and quality improvement purposes. In this study, we quantified the frequency and pattern of synoptic reporting by pathologists in VA Medical Centers across the United States for bladder and kidney cancers.
Methods:We conducted this study using data from the VA nationwide Corporate Data Warehouse (CDW) from 2019 through 2022. We randomly sampled a minimum of 200 biopsy and 200 resection pathology reports for each cancer type, totaling 802 reports. Trained annotators manually reviewed these reports to determine whether a synoptic report was issued. Synoptic reports were further scrutinized to ensure that all core elements were adequately documented. Analysis of Variance (ANOVA) was used to compare the mean of the proportions of core elements that were documented across cancer types. Finally, within each cancer type, the frequency of each core element that was reported was also recorded.
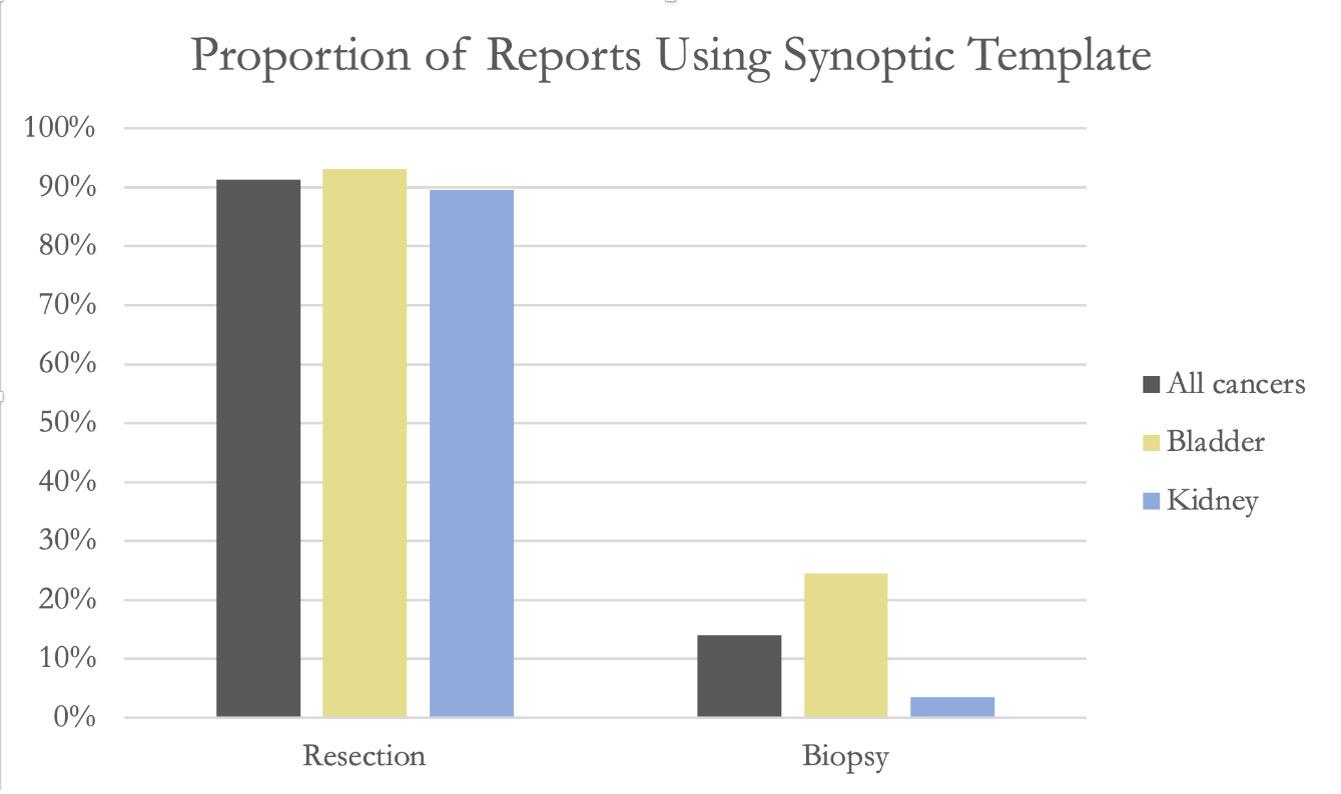
Results:Synoptic reporting templates were used in 423 (53%, 95% CI 49%-56%) of the 802 reviewed reports. Synoptic reporting was significantly more common among bladder than kidney cancers at 237 of 402 compared to 186 of 400, respectively (59% vs 46%, ANOVA p < 0.001). Synoptic reporting was much more common among resection reports than among biopsy reports (91% vs 14%, ANOVA p < 0.001. It was used least frequently among kidney biopsy reports (3.5%, 95% CI 1.7% - 7%) (Fig. 1). Among kidney resections, core elements were completed more than 91% of the time, with “rhabdoid features” being the most frequently missing core element. Among the 49 synoptic reports issued for bladder biopsies, “tumor site” was most often missing (24%, 95% CI 18% - 38%). Nevertheless, when synoptic templates are used, the overwhelming majority of required information is reported.
Conclusions:In this study we reveal insights into the written communication between pathologists and clinicians. In general, synoptic reporting is used far more for resections than biopsies. This is perhaps because accreditation from the College of American Pathologists and the Joint Commission requires synoptic templates for resections but not biopsies. Synoptic reporting results in most core elements being reported. Taken together, our results suggest that expansion of currently available synoptic reporting for biopsies could help standardize communication. We hope that standardization would facilitate more accurate and efficient communication among clinicians and pathologists.
Figure 1