BACKGROUND: There has been a recent surge in clinical trials focused on patients who have recurrent disease of their non-muscle-invasive bladder cancer (NMIBC) after Bacillus Calmette-Guérin (BCG). Due to ongoing BCG shortages and access to alternative agents, the true number of patients who are receiving BCG induction is unclear. Herein, we evaluated this question and elucidated alternative treatment agents that patients received among a contemporary US insurance claims database.
METHODS: From the Komodo Health claims database (1/2018-3/2023) with Medicare Advantage, Medicaid, Managed Medicaid, and commercially insured patients, we identified patients with NMIBC using the following algorithm: a) presence of carcinoma in situ (CIS), or b) presence of bladder cancer (BC) and transurethral resection of bladder tumor, followed by intravesical chemotherapy or immunotherapy or 12 months with no treatment and no evidence of muscle-invasive BC. Patients were further queried to identify those who received adequate BCG induction (ie, ≥5 weekly instillations). We summarized the distribution of this group and the treatments following BCG induction with ≥12 months of evaluable data for the overall population and the CIS subgroup.
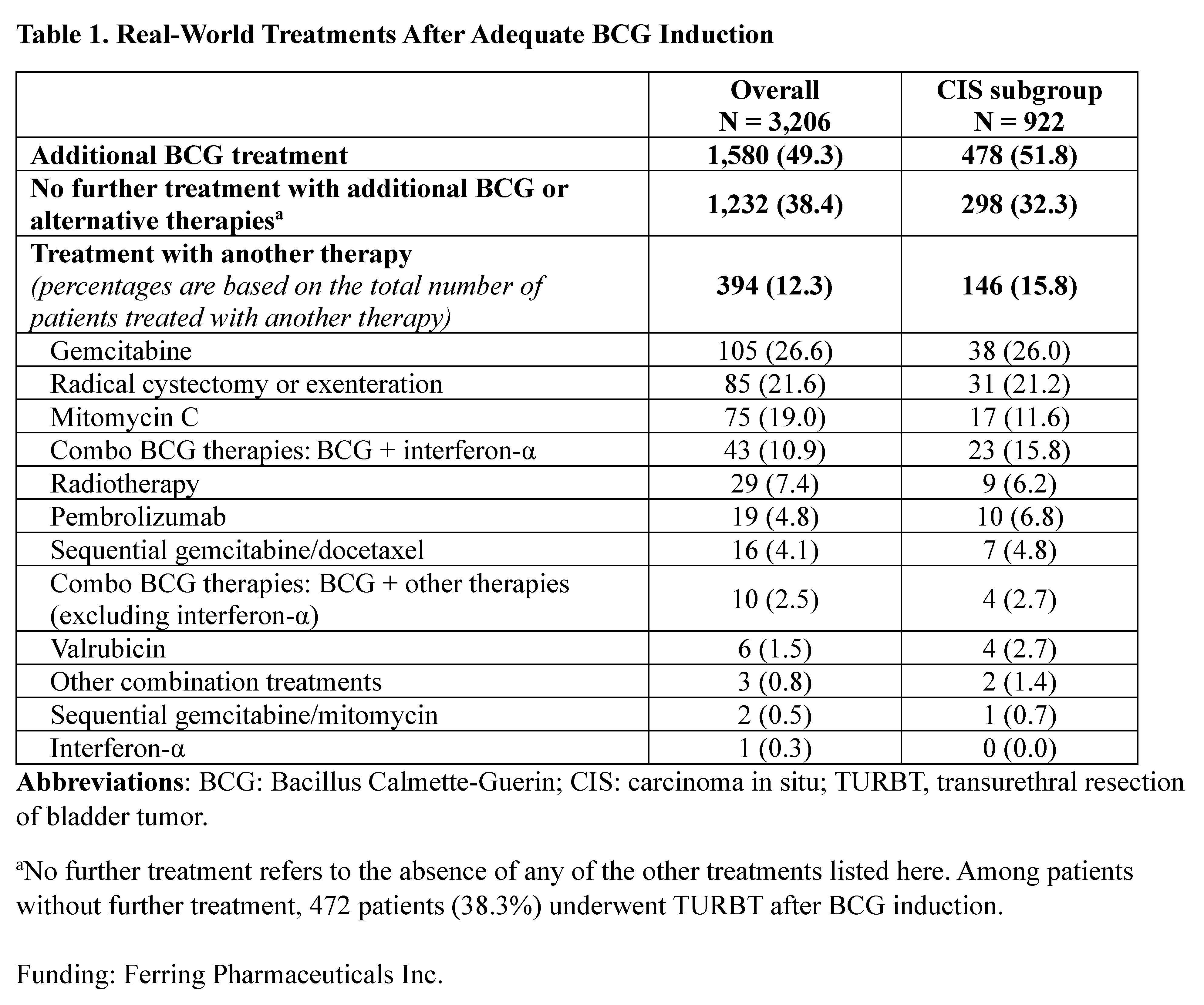
RESULTS: Of 7,058 patients with NMIBC receiving BCG, more than half (4,478, 63.4%) had adequate BCG induction; of these patients, 3,206 had ≥12 months data (including 28.8% patients with CIS). Following adequate BCG induction, 49.3% had further BCG and 24.9% had ≥2 doses of maintenance BCG; 38.4% had no further treatment, and 12.3% (394 patients) were treated with other therapies - including gemcitabine (26.6%), radical cystectomy or exenteration (21.6%), mitomycin C (19.0%), BCG + interferon-α (10.9%), radiotherapy (7.4%), and pembrolizumab (4.8%). A similar distribution was observed in the CIS subgroup though BCG + interferon-α was the third most common treatment (Table 1).
CONCLUSIONS:In this analysis, we found that more than half of patients with NMIBC treated with BCG received adequate BCG induction but only one-quarter received maintenance BCG. Among patients who received other therapies after induction, gemcitabine, radical cystectomy or exenteration, and mitomycin C were the most commonly used. These patterns have implications not only for patient care, but especially for clinical trial design and enrollment.