BACKGROUND: Several randomized trials have reported improved recurrence rates with a single, postoperative instillation of intravesical chemotherapy (POC) after transurethral resection of bladder tumor (TURBT). Accordingly, clinical practice guidelines recommend POC for suspected low- or intermediate-risk bladder cancer to reduce recurrence rates. However, real-world data on the effectiveness of POC are lacking, particularly in older adults, and clinical adoption remains low. We therefore emulated a completed randomized trial to provide contemporary, real-world data on the comparative effectiveness of POC after TURBT, and examined clinicopathologic features associated with its utilization.
METHODS: We conducted observational analyses to emulate SWOG 0337 in older adults. We identified patients aged 66-74 years with cTaN0M0 urothelial carcinoma of the bladder treated with TURBT with or without POC (gemcitabine or mitomycin C) from 2000-2017 in SEER-Medicare. After estimating a propensity score for treatment, we evaluated the association of POC with recurrence-free (RFS) and progression-free survival (PFS) using inverse probability of treatment weights (IPW). Recurrence and progression events were assessed using Medicare claims. We also examined the association of POC utilization with baseline characteristics using multivariable regression.
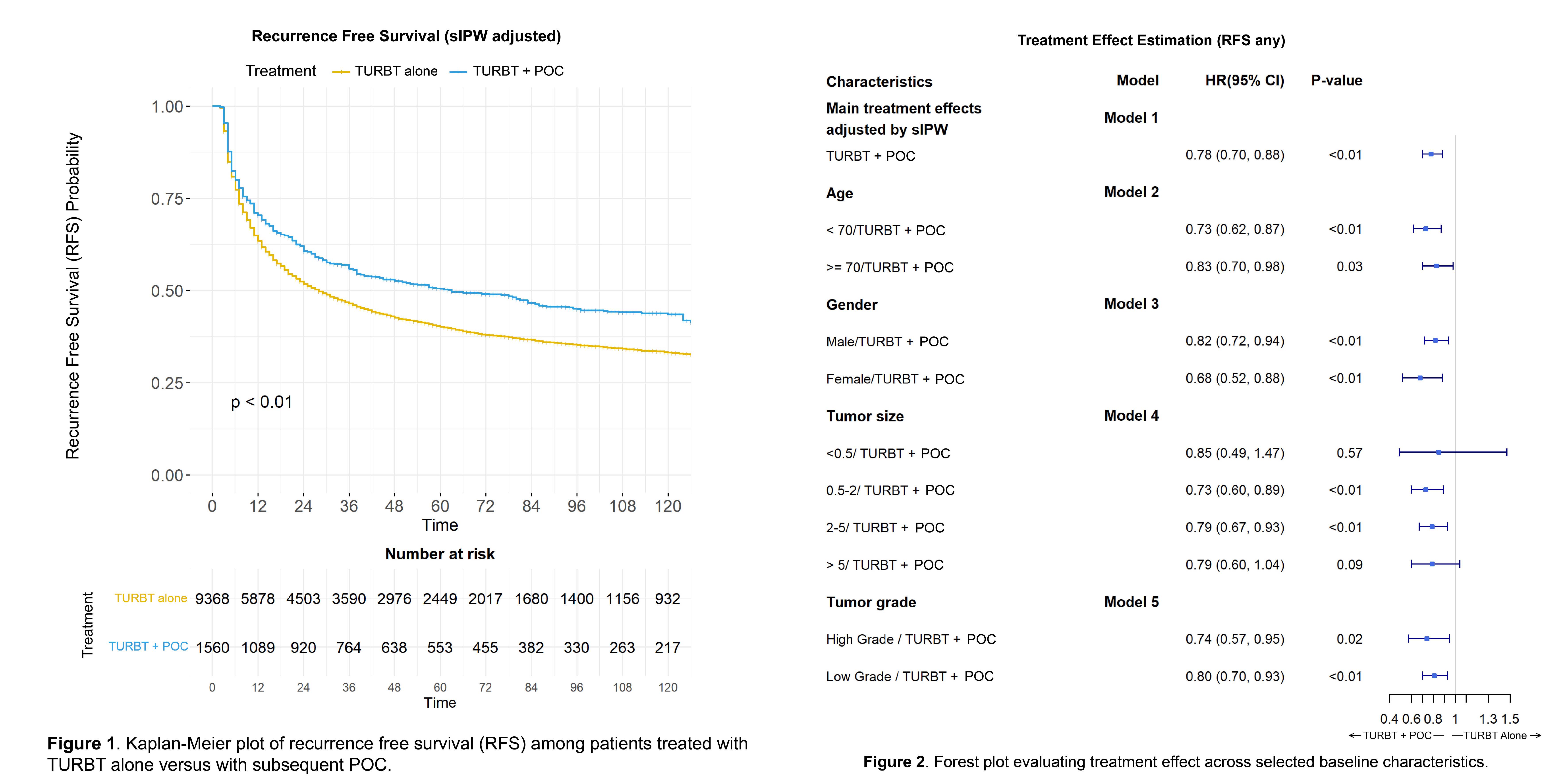
RESULTS: A total of 10,917 patients were included in the study cohort, of whom 9,367 (86%) were treated with TURBT alone and 1,550 (14%) with TURBT + POC. After IPW-re-weighting, baseline characteristics were balanced. Median follow-up was 87.0 (IQR 47.0-139.0) months, during which time 6,486 recurrences and 564 progression events occurred. After IPW adjustment, TURBT + POC was associated with improved RFS compared to TURBT alone, with 5-year RFS of 50% vs 40% (HR 0.78, 95% CI 0.70-0.88, p<0.01), respectively (Figure 1). Notably, TURBT + POC was associated with improved RFS when examining heterogeneity of treatment effects across tumor size and tumor grade (Figure 2), suggesting a benefit regardless of tumor grade and size. However, TURBT + POC was not associated with a difference in PFS compared to TURBT alone (p=0.39). In multivariable analyses examining receipt of POC, later year of diagnosis (OR 20.1, 95% CI 14.8-27.2 for 2015-2017 vs 2000-2003), higher zip code income (OR 1.36, 95% CI 1.06-1.76), and higher education level (OR 1.38, 95% CI 1.05-1.81 for <14% without high school education compared to >29%) were associated with increased odds of receiving POC, while older age (OR 0.97, 95%CI 0.95-0.99) was associated with lower odds of receiving POC.
CONCLUSIONS:
In observational analyses using real-world data to emulate a completed target trial, POC after TURBT was associated with improved RFS, irrespective of tumor grade or size, but not improved PFS. However, POC remains underutilized, with older patients and those from lower education or lower income areas less likely to receive it. These findings highlight the need to improve utilization of POC and investigate potential disparities related to its use.