Introduction: Intracavernosal injection (ICI) therapy for erectile dysfunction (ED) carries a risk of corporal fibrosis, possibly making implantation of inflatable penile prosthesis more difficult and increasing the risk of postoperative complications related to poor corporal integrity.
Methods: A retrospective cohort study of primary IPP cases from 2016-2021 across 16 institutions. Patients were stratified by history of ICI and between-group differences in risk factors were assessed by univariate analysis. Multivariable logistic regression was used to assess for predictors of intraoperative complications (corporal perforation, urethral injury), and postoperative complications related to poor integrity of corporal tissue including cylinder migration, deviation, herniation, erosion and glans deformity.
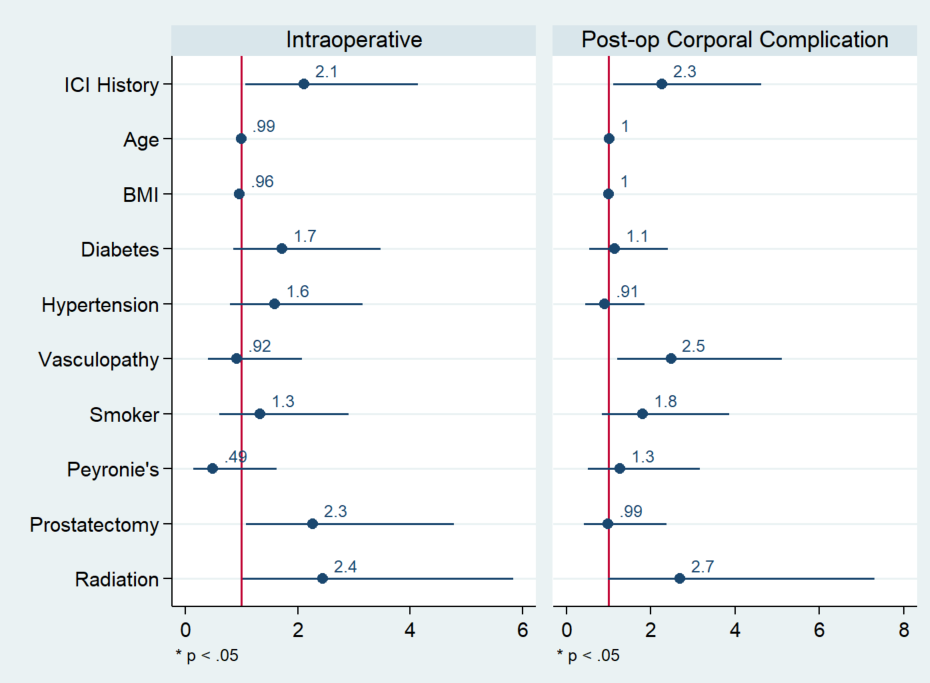
Results: A total of 2495 patients met inclusion criteria of which 781 (30.8%) had a history of ICI. On univariate analysis Patients with a history of ICI tended to be older (mean 63 vs 64 years, p=0.002) and were more likely to have history of radical prostatectomy (21.0% vs. 32.1%, p<0.001) and/or radiation (5.5% vs 10.9%, p<0.001), and less likely to have a history of Peyronie�s (18.9% vs 14.7%, p=0.012). 32 patients (1.3%) had postoperative complications related to poor corporal integrity, with a significant increase in the rate on univariate analysis (0.009% vs 0.02%, p 0.011). On multivariable regression, a history of ICI, prostatectomy, and radiation were all significant predictors of intraoperative complications (OR 2.11, p=0.03; OR 2.27, p=0.03; OR 2.40, p=0.04, respectively). A history of ICI and a history of vasculopathy were both independent predictors of postoperative complications related to poor corporal integrity (OR 2.27, p=0.02, OR 2.48, p=0.014 respectively).
Conclusions: In men undergoing IPP placement, a history of ICI is associated with an increased risk of both intraoperative and postoperative complications related to poor corporal integrity. In addition to ICI history, prostate cancer treatment with radiation or surgery is independently associated with increased risk of intraoperative complications, while a history of vasculopathy is an independent predictor of poor corporal integrity post-op. These findings may help guide patient selection and shared decision making and support the notion that ICI therapy may be inappropriate in some patients.