BACKGROUND: We report bladder function and safety from a phase 3 trial of vibegron, a selective β3-agonist under investigation for use in men with persistent OAB symptoms who are being pharmacologically treated for BPH.
METHODS: COURAGE (NCT03902080) was a 24-week, phase 3, multicenter, randomized, double-blind, placebo-controlled trial. Men ≥45 years with OAB and BPH receiving a stable dose of α-blocker � 5α-reductase inhibitors were randomized 1:1 to once-daily vibegron 75 mg or placebo. Urodynamic evaluations of Qmax during voiding and detrusor pressure at peak flow rate (PdetQmax) were collected at baseline and week 12 from patients with evaluable parameters at baseline and ≥1 parameter postbaseline (urodynamics evaluable set [UES]). From the safety analysis set (SAF), postvoid residual (PVR) urine volume, maximum urinary flow rate (Qmax) as measured by uroflowmetry (Uroflow Qmax; at baseline and Week 24), and urological adverse events (AEs) were collected. Urinary retention (≥200 mL to <300 mL with symptoms or ≥300 mL regardless of symptoms), residual urine volume increase (elevated PVR volume considered clinically significant by investigator), urinary tract infection (UTI), and cystitis were collected as protocol-defined AEs of special interest (AESIs).
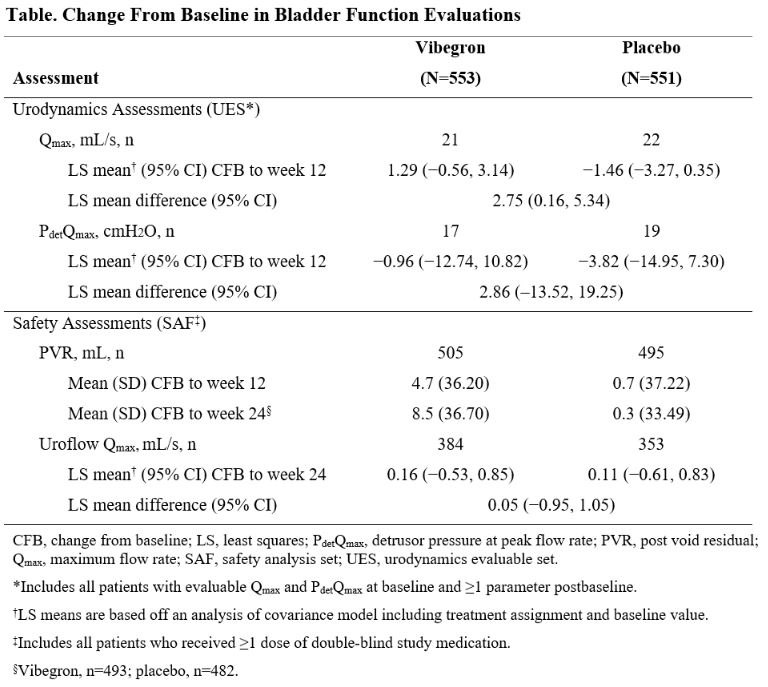
RESULTS: Overall, 1104 patients (vibegron, n=553; placebo, n=551) were included in the SAF. The UES (vibegron, n=21; placebo, n=22) consisted of 43 patients. The mean (SD) duration of treatment was 156.7 (36.4) days for vibegron and 155.6 (37.3) days for placebo. In the UES, the least squares mean difference (LSMD; 95% CI) between groups in change from baseline (CFB) at week 12 in Qmax was 2.75 (0.16, 5.34) mL/s (Table). Vibegron was noninferior to placebo for CFB at week 12 in Qmax (lower limit of the 1-sided 95% CI for the treatment difference was greater than the noninferiority margin of -3 mL/s). LSMD (95% CI) between groups in CFB at week 12 in PdetQmax was 2.86 (-13.52, 19.25) cmH2O. In the SAF, differences in PVR and Uroflow Qmax were minimal between treatment groups at week 24. In the SAF, AEs of urinary retention were reported for 5 (0.9%) and 4 (0.7%) patients in the vibegron and placebo groups, respectively. Notably, 8 of 9 cases had ≥1 risk factor for retention (Uroflow Qmax <12 mL/s, prostate volume ≥40 mL, prostate-specific antigen ≥1.4 ug/L) at baseline, and ≥2 occurred following events unrelated to OAB/BPH (motor vehicle accident, spinal surgery; both vibegron group). Residual urine volume increase was reported in 1 (0.2%) and 3 (0.5%) patients receiving vibegron and placebo, respectively. UTI was reported in 14 (2.5%) and 12 (2.2%) patients, respectively; 0 and 1 patient reported cystitis. No AEs of urinary retention or residual urine volume increased were reported in the UES.
CONCLUSIONS: In men with residual OAB symptoms and pharmacologically treated BPH, no unexpected safety signals related to bladder function were noted with once-daily vibegron, and there were no differences in bladder function between vibegron and placebo.