


Elevated CRP after Radical Cystectomy is Associated with Infectious, Wound, and Anastomotic Complications
Joshua A. Linscott, MD, PhD, Randie E. White, MD, Stephen T. Ryan, MD, Moritz H. Hansen, MD, Matthew H. Hayn, MD, Jesse D. Sammon, DO.
Maine Medical Center, Portland, ME, USA.
BACKGROUND: Radical cystectomy (RC) is a highly morbid procedure with frequent infection related complications and readmissions. CRP is a non-specific inflammatory marker often used to guide patient management, with reported indications in the post-operative period. We hypothesized that a markedly elevated CRP several days after RC may be a sub-clinical indicator of complication risk due to infection, wound breakdown, or anastomotic leak
METHODS: Our prospectively maintained database included CRP starting May, 2020. For 66 consecutive patients, 58 had CRP measured POD#4. Fever or leukocytosis (WBC >11.0) after POD#4 was also recorded. Complications were graded and classified by the MSKCC system. CRP was compared between patients with 30d Infectious/wound/anastomotic leak (I/W/A) complications and those without. ROC analysis was used to determine the optimal cutoff for elevated CRP. Multivariable analysis was performed to find factors associated with I/W/A complications
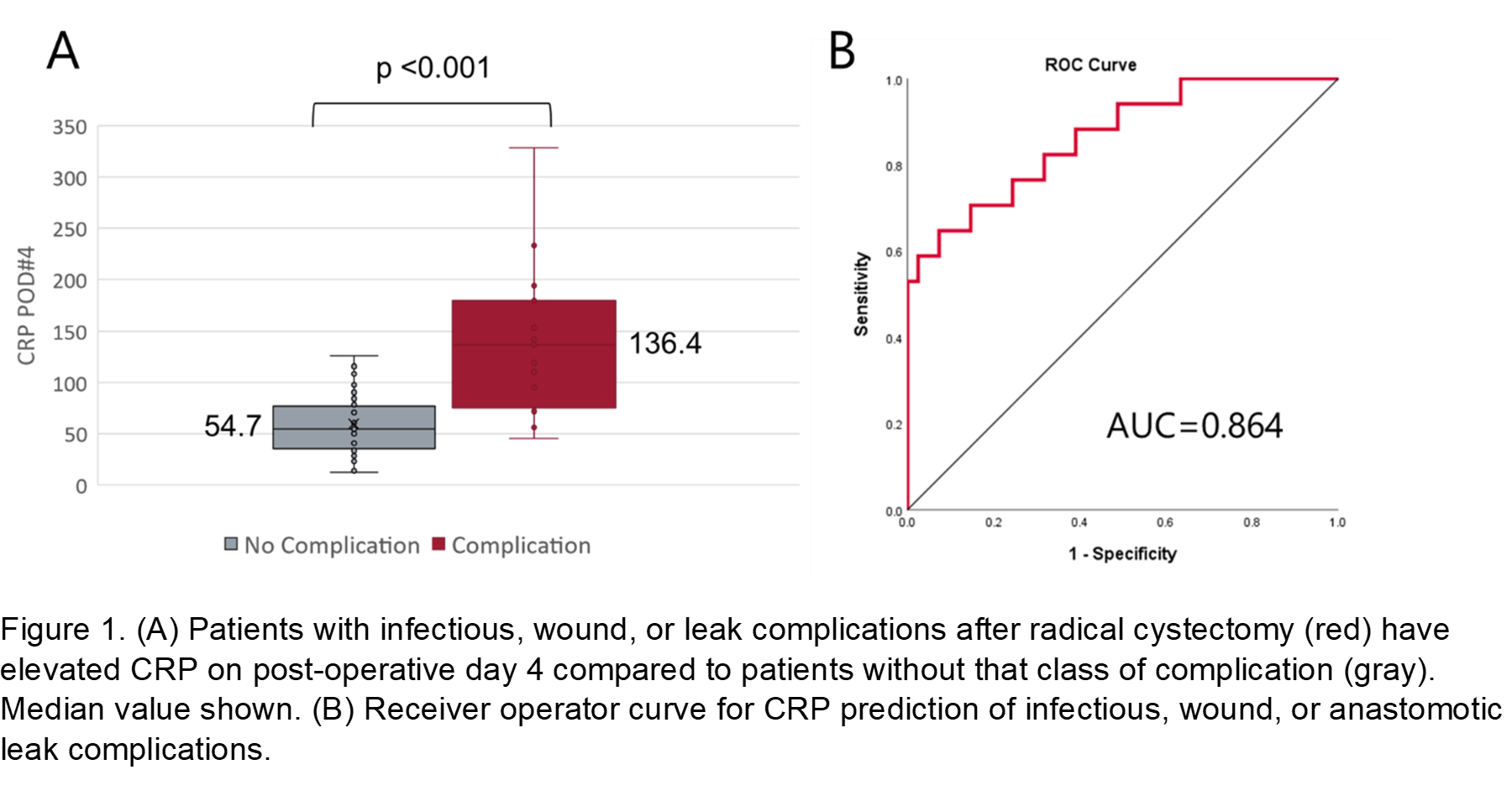
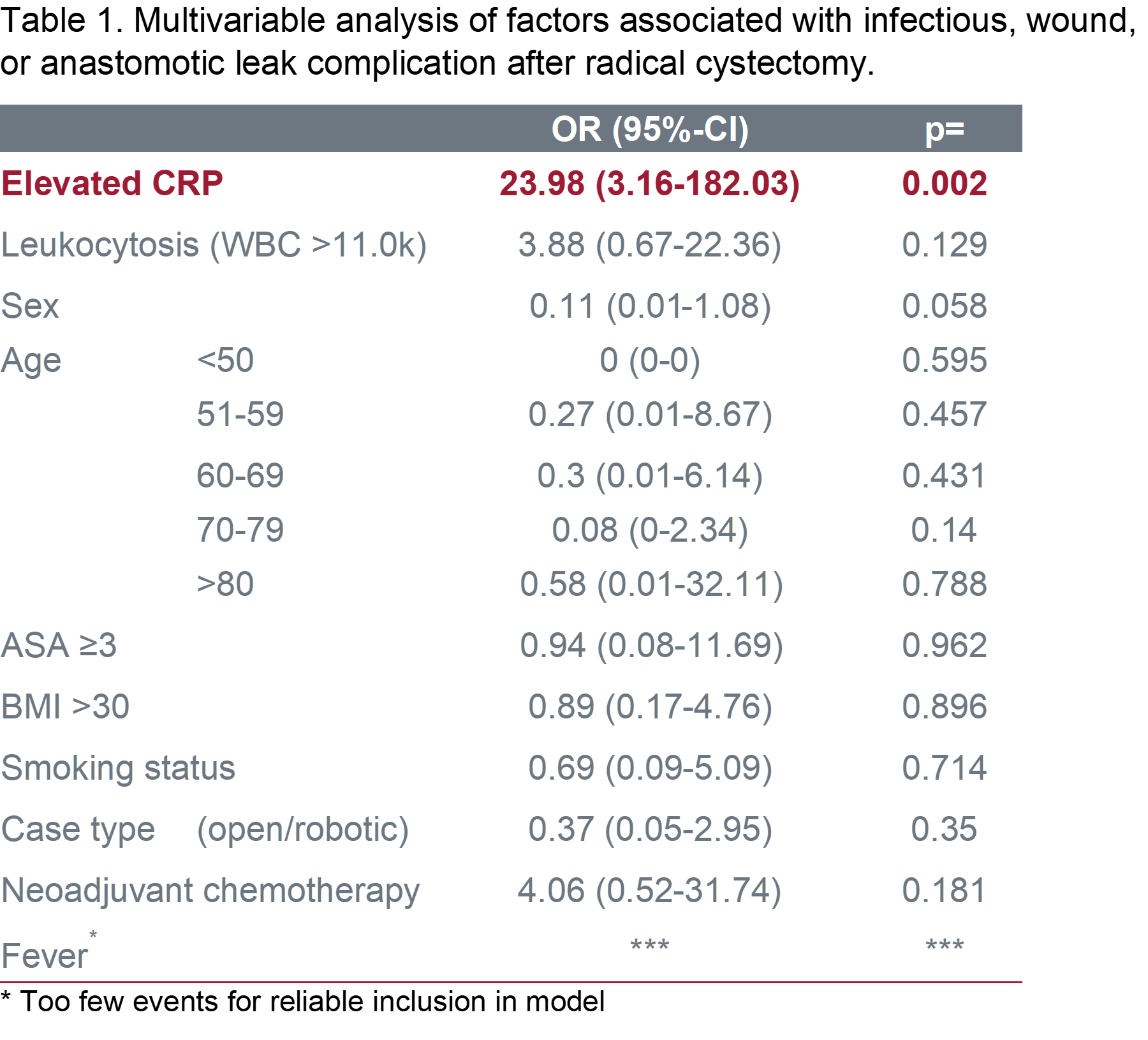
RESULTS: Median CRP for patients with I/W/L complications was 136.4 vs 54.7 for those without (Figure 1). No significant differences in demographics were seen between groups. CRP performed well on ROC analysis for I/W/A with an AUC = 0.864 and a CRP of 93 chosen as a cutoff for being elevated based on Youden's index (Figure 1). Adjustment for disease burden, postop fever, leukocytosis, treatment type, and demographic characteristics showed only elevated CRP was independently associated with I/W/A complications (OR23.98, 95%CI 3.16-182.03, p=0.002, Table 1).
CONCLUSIONS: Preliminary data suggests that CRP elevation on POD#4 can be a sub-clinical marker of future I/W/A complications within 30 days following RC. This association independent of other markers of infection including leukocytosis and fever (which was rare). There should be high suspicion of I/W/A complication for patients with an elevated CRP and modified discharge pathways or closer follow-up may be one a future strategy to try and prevent or reduce this morbidity.
Back to 2022 Abstracts