


The association of baseline frailty with survival among older adults undergoing radical cystectomy for bladder cancer.
John Ernandez, BA1, Sumedh Kaul, MS2, Aaron Fleishman, MPH2, Ruslan Korets, MD3, Peter Chang, MD, MPH3, Andrew Wagner, MD3, Simon Kim, MD4, Joaquim Bellmunt, MD, PhD5, Nima Aghdam, MD6, Aria Olumi, MD3, Dae Kim, MD, MPH, ScD7, Boris Gershman, MD3.
1Harvard Medical School, Boston, MA, USA, 2Department of Surgery, Beth Israel Deaconess Medical Center, Boston, MA, USA, 3Division of Urologic Surgery, Beth Israel Deaconess Medical Center, Boston, MA, USA, 4Division of Urology, University of Colorado Anschutz Medical Center, Aurora, CO, USA, 5Department of Medicine, Division of Medical Oncology, Beth Israel Deaconess Medical Center, Boston, MA, USA, 6Department of Radiation Oncology, Beth Israel Deaconess Medical Center, Boston, MA, USA, 7Marcus Institute for Aging Research, Hebrew SeniorLife, Boston, MA; Division of Gerontology, Department of Medicine, Beth Israel Deaconess Medical Center, Boston, MA, USA.
BACKGROUND: Frailty is increasingly recognized as an important component of geriatric assessment in older adults and an important predictor of clinical outcomes. We hypothesized that baseline frailty is an independent predictor of survival for older adults undergoing radical cystectomy (RC) for bladder cancer. Herein, we examined the associations of a validated, claims-based frailty index (CFI) with survival in a large, population-based cohort.
METHODS: Using the SEER-Medicare linked database, we identified older adults aged 66-89 years diagnosed with Tany Nany cM0 urothelial carcinoma of the bladder from 2000-2017 who underwent RC. Baseline CFI was calculated using a 12-month pre-diagnosis period. The associations of CFI with survival outcomes were assessed using the Kaplan-Meier method and Cox multivariable regression.
RESULTS: A total of 5,916 patients were included in the study cohort, including 3,389 who were robust (CFI <0.15), 2,247 who were pre-frail (CFI 0.15 to <0.25), 232 who were mildly frail (CFI 0.25 to <0.35), and 48 who were moderately-to-severely frail (CFI ≥0.35). Median follow-up was 37.0 (IQR 16.0-84.0) months. During follow-up, a total of 3,998 deaths occurred. Before adjustment, increasing level of frailty as reflected by the CFI was associated with worse cancer-specific survival, other-cause survival, and overall survival (Figure 1). In multivariable modelling, increasing CFI was independently associated with worse all-cause mortality, cancer-specific mortality, and other-cause mortality (Table 1).
CONCLUSIONS: Among older adults undergoing RC for bladder cancer, increasing baseline frailty as measured by the CFI was associated with worse survival outcomes, even after adjustment for patient and tumor characteristics. The CFI provides an objective assessment that can be used to improve decision-making in older adults with bladder cancer. 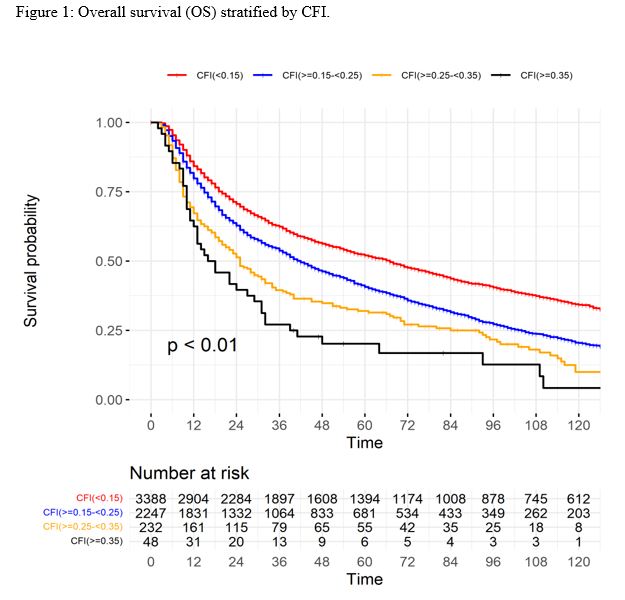

Back to 2022 Abstracts