


Urinary Thiosulfate Level in Stone Forming Versus Non-Stone forming Pregnant Females
Shuo-chieh Wu, MD1, Eileen Brandes, MD1, John Asplin, MD2, Vernon Pais, MD3.
1Dartmouth-Hitchcock Medical Center, Lebanon, NH, USA, 2LithoLink Corp, Chicago, IL, USA, 3Dartmouth-Hichcock Medical Center, Lebanon, NH, USA.
BACKGROUND:
Renal colic is the most common cause of non-obstetric hospitalization in the pregnant patient. Pregnancy is associated with multiple metabolic changes, including increased excretion of urolithiasis promoters including sodium, calcium, and uric acid. Prior study has established increased urinary calcium chelators in the third trimester of pregnancy. This phenomenon is thought to be a physiologic protective mechanism against the urolithiasis promoters. One such example is urinary citrate, which increases and decreases with urinary calcium level at different stages of pregnancy. Thiosulfate is a chelating agent that has also been associated with protective effect against calcium stone formation in animal models. Our study measured urinary thiosulfate on a controlled diet during third trimester and the postpartum period and sought to assess whether exogenous thiosulfate could serve as a viable lithogenic protective agent.
METHODS:
We recruited a cohort of pregnant patients between year 2014-2019, and collected 24-hour urine samples with IRB approval. The urine samples were collected from patients on a standardized diet at third trimester, post-partum, and post-lactation stages. Patients were identified as new stone formers during pregnancy or non-stone formers based on review of history. Urinary thiosulfate and other chemical components at various stages of pregnancy were analyzed.
RESULTS:
We recruited a total of 14 pregnant patients without history of stones prior to gestation. In order to control for dietary-induced variation in urine chemistry, all patients were placed on a standardized diet for the day before and day of each collection. Twenty-four hour urine was submitted third trimester (n = 14), post-partum (n = 12), and post-lactation (n = 6) stages. A total of 4 patients had new stone formation during pregnancy. Urinary calcium was noted to be increased in the third trimester (p = 0.01) with corresponding increase in the urinary citrate (p = 0.02). However, there was no statistical difference (p = 0.97) of urinary thiosulfate across third trimester (13.89 mEq, IQR 9.1 - 19.71), post-partum (13.87 mEq, IQR 8.6 - 20.5), and post-lactation (14.53 mEq, IQR 7.7 - 20.9) stages. Stratified analysis showed no statistically significant difference in thiosulfate level between stone former versus non-stone formers.
CONCLUSIONS:
Unlike urinary citrate and calcium, endogenous urinary thiosulfate does not change significantly from the third trimester of pregnancy to post-partum stage in our cohort of patients on a standardized diet. Our observation does not support urinary thiosulfate as a lithogenic protective factor or utilization of exogenous thiosulfate as a strategy to prevent stone formation. 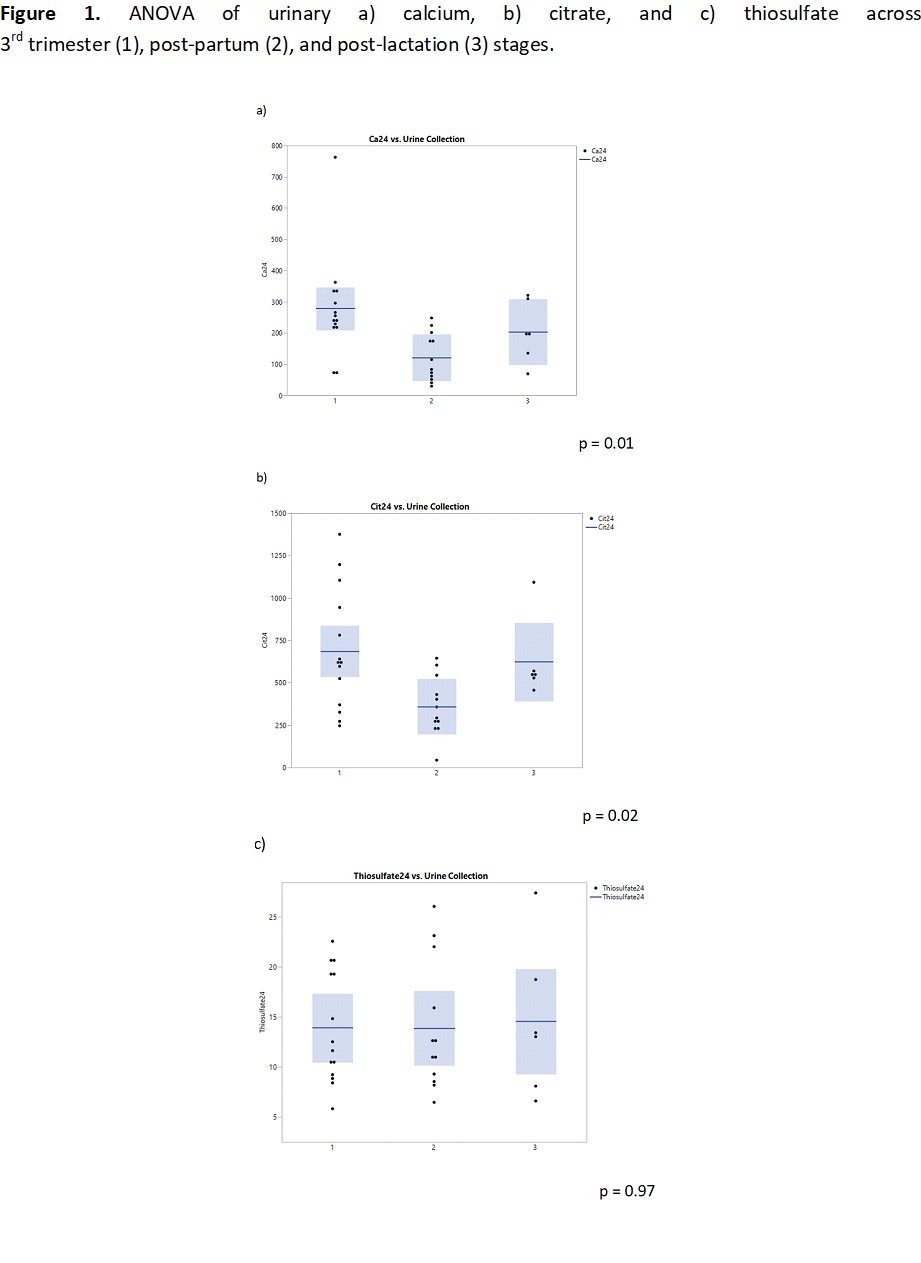
Back to 2022 Abstracts