


Patient Expectations after Robot-Assisted Laparoscopic Prostatectomy
Yuchen Liu, BS & BA, Kola Olugbade, MD, Allison Kleeman, BS, Jeffrey Sun, BS, Catrina Crociani, MPH, May Jean Counsilman, MD, Andrew A. Wagner, MD, Peter Chang, MD.
Beth Israel Deaconess Medical Center, Boston, MA, USA.
BACKGROUND: In prior studies, prostate cancer (PC) patients undergoing robot-assisted laparoscopic prostatectomy (RALP) were more likely to be regretful and dissatisfied than those who underwent open radical prostatectomy. The degree of urinary incontinence and postoperative erectile dysfunction were predictors of regret. We hypothesize that there exist discrepancies between patients' expectations and their actual outcomes and that these discrepancies are associated with decisional regret. In this study, we aim to understand patients' expectations of recovery, how their expectations differ from reality, and if such discrepancies predict being regretful of undergoing RALP.
METHODS: The Expanded Prostate Cancer Index Composite for Clinical Practice (EPIC-CP) is a 16-item questionnaire assessing PC patients' health-related quality of life (HRQOL) at the point of care. A higher EPIC-CP score indicates worse HRQOL. Sixty-one subjects between 2019 to 2021 were prospectively enrolled in this IRB-approved study. Prior to surgery, we had subjects estimate their 3- and 12-month post-operative HRQOL by completing �predictive� EPIC-CP questionnaires - these represented patients' expectations. The subjects then underwent RALP, and completed EPIC-CP 3- and 12-months after surgery, which constituted their actual HRQOL outcomes. We then used the Wilcoxon Rank Sum Test to evaluate whether there were statistically significant differences between the anticipated and actual recovery for each HRQOL domain at 3- and 12-months post-surgery. The Decision Regret Scale, a validated five-item questionnaire used to measure the level of regret, was completed by participants at 12-months. We used Fisher's Exact Test to assess whether a worse-than-anticipated recovery was associated with regret.
RESULTS: At 3-months, the mean HRQOL was better than what subjects expected (mean expected - observed EPIC-CP scores were significantly higher in the urinary incontinence, urinary irritation/obstruction, vitality, and hormonal domains; see Table 1). At 12-month post-operatively, however, discrepancies between expectations and reality in the prior-mentioned HRQOL domains were no longer significant, and subjects' sexual HRQOL was worse than they had anticipated (mean expected - observed EPIC-CP sexual scores was -2.43; p < 0.01; Table 1). In other words, on average, subjects expected their sexual HRQOL to be better than it actually was 12 months post-operatively. We found that subjects who experienced a worse-than-anticipated recovery at 12-months were more likely to regret undergoing RALP (p = 0.042).
CONCLUSIONS: Discrepancies between subjects' HRQOL expectations and actual outcomes are common after RALP. At our institution, 3-month HRQOL outcomes were better than subjects' expectations. However, many subjects expected their sexual HRQOL recovery at 12-months to be further along than their actual outcome. The discrepancy between expectations and reality was associated with decisional regret, highlighting the importance of pre-treatment patient counseling in accurately adjusting patient expectations. Strategies to reduce these discrepancies may include the use of validated decision aids and should be the subject of further study. 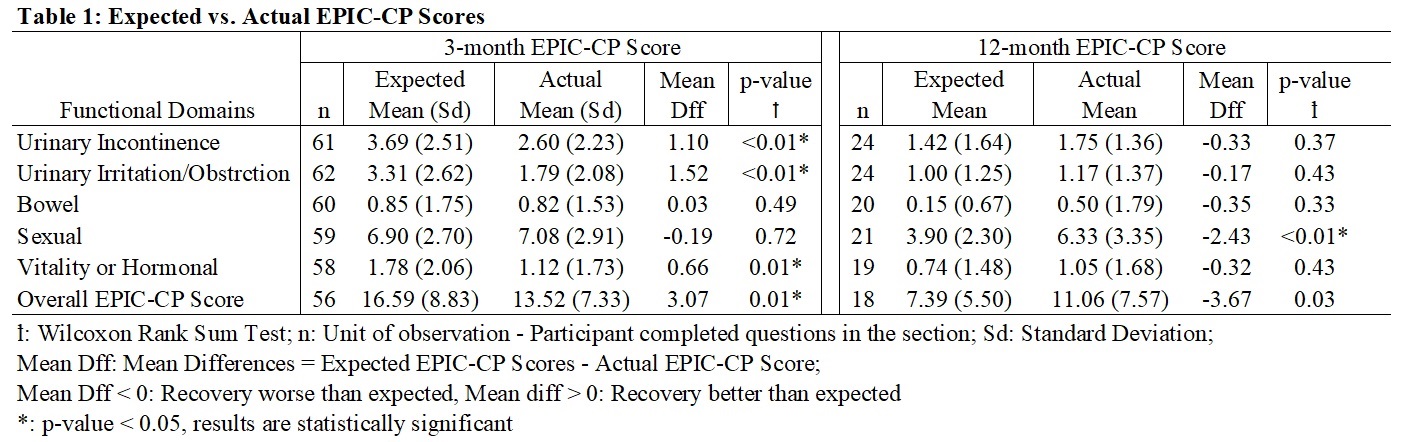
Back to 2022 Abstracts