


Provider-level and regional variation in robotic-assisted laparoscopic prostatectomy volume
Jacob Abraham, Alexander Homer, Rebecca Ortiz, Faizanahmed Munshi, Elias Hyams
Minimally Invasive Urology Institute, The Miriam Hospital, Providence, RI, USA.
BackgroundThere is a well-established relationship between surgical volume and perioperative and oncological outcomes for robotic-assisted laparoscopic radical prostatectomy (RALP). [1] However, there is limited recent evidence regarding variation in surgical volume at the surgeon and regional level.[2] In this study, we evaluated variation in RALP volume among Medicare patients to better understand recent practice patterns and inform discussions on centralization of care.
MethodsUsing publicly available Medicare data (https://data.cms.gov/) we determined the number of RALPs (CPT 55866) performed by urologists in the United States from 2014-2019. Providers were grouped into 4 United States regions by state: West, Midwest, Northeast, and South. The data were analyzed descriptively and using a multiple linear regression model with region fixed effects to determine the difference in provider RALRP volume across regions. Data were censored for provider volume <11 cases / year due to privacy concerns.
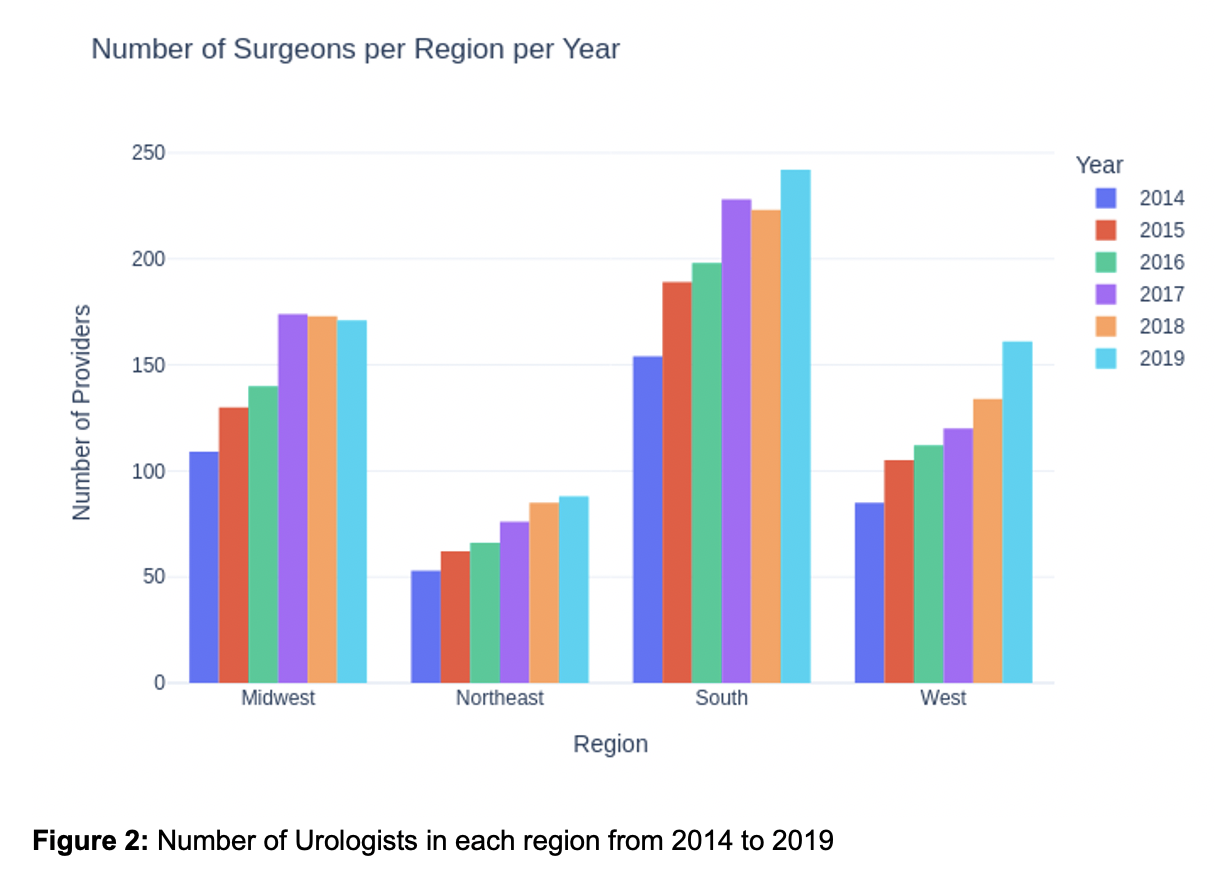
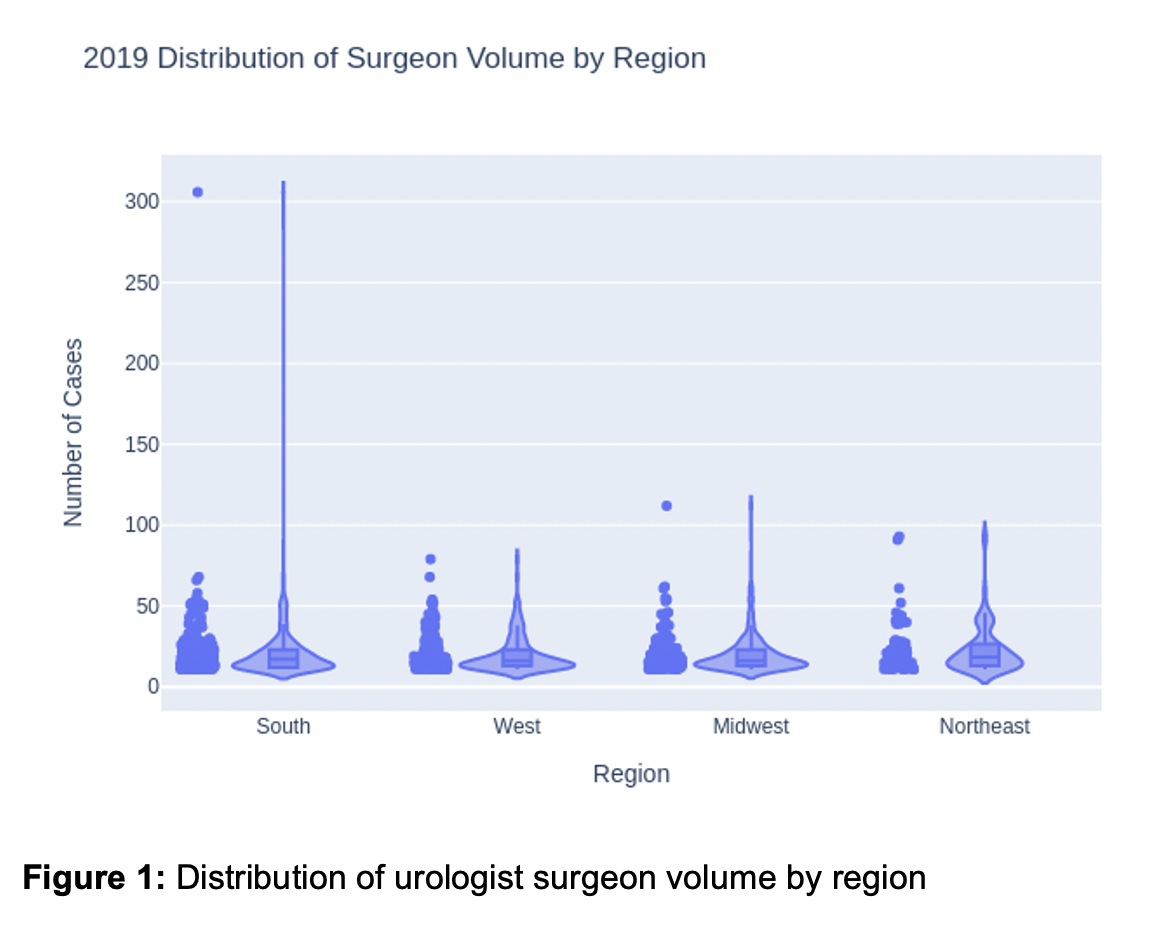
ResultsDuring the study period, there were 1058 distinct providers performing RALP in Medicare patients. Mean surgical volume per provider per year was 21.09 (SD 16.46, IQR 11). The highest and lowest surgical volume per provider were 306 and 11 cases, respectively (Figure 1). There were significant regional differences in RALP volume per physician with highest volume in the Northeast (Figure 3A), despite outlying high volume providers (Figure 1). There was an increasing number of RALPs performed over time, but no change in procedures per physician per year (Figure 2/3).
ConclusionsIn recent Medicare data, there is wide variation in RALP volume at the provider and regional level. While this is a subset of overall surgical practice, these data elicit questions regarding the frequency of lower volume surgery and the consideration of centralization to improve outcomes. [3] Further research is needed to determine how to centralize surgical treatment of prostate cancer most effectively.
Figure 1: Distribution of urologist surgeon volume by region
Figure 2: Number of Urologists in each region from 2014 to 2019
Figure 3A: Mean Number of Procedures per Physician in each Region and Year
Figure 3B: Mean Number of Procedures per Physician in each Region and Year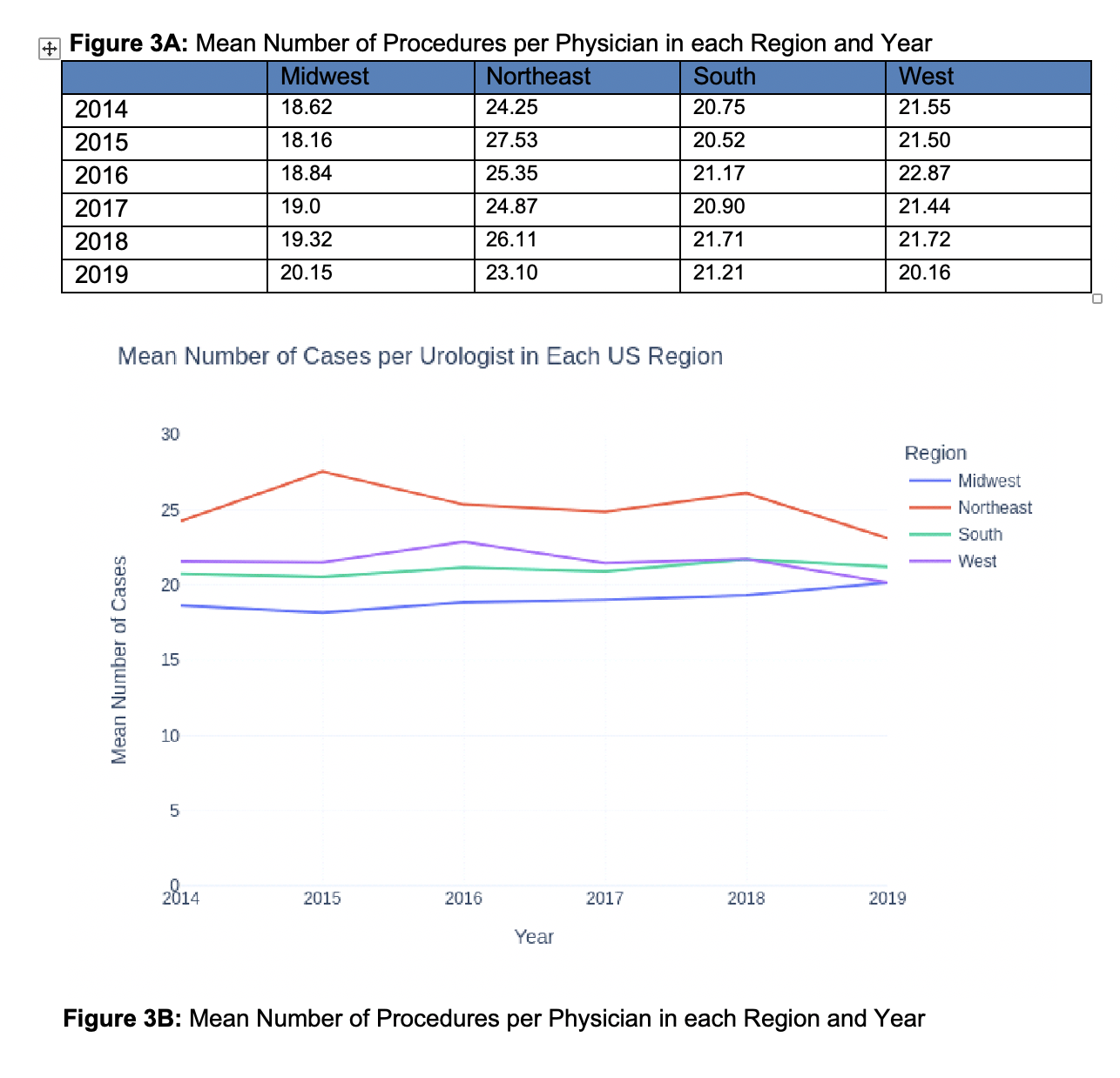
Back to 2022 Abstracts