


Risk Stratification Using A Polygenic Risk Score Improves PSA Screening Efficiency: An Analysis of the PCPT Cohort
Mitchell Nguyen, MD1, Stephen Ryan, MD1, Fady Ghali, MD2, Vi Nguyen, MD3, Brandie Heald, MS4, Edward D. Esplin, MD, PhD4, Michael Liss, MD5, Andrew Kader, MD, PhD3.
1Maine Health, Portland, ME, USA, 2University of Washington, Seattle, WA, USA, 3University of California San Diego, San Diego, CA, USA, 4Invitae, San Francisco, CA, USA, 5UT Health, San Antonio, TX, USA.
Background Prostate-specific antigen (PSA) based prostate cancer (PCa) screening reduces PCa related mortality, however, universal PSA screening (UPS) leads to unnecessary interventions, complications, and actions for many men who will, ultimately, never be diagnosed with PCa. Genetic risk-stratification, using a polygenic risk score (PRS), may play a role in better targeting PSA screening and improving screening efficiency (e.g. number of screening events required to detect PCa). Using data from the placebo arm of the PCa Prevention Trial (PCPT), we compared the screening efficiency of several risk adapted and non-risk adapted hypothetical screening models.Methods Efficiency was assessed by determining the number of screening events that each screening model would generate and what percentage of overall and high grade cancers would be diagnosed. In the UPS model all men are screened. In the family history (FH) model, only men with a FH of PCa would be screened. Finally, the PSA >1 and >1.5 models would only screen those men with PSAs greater than those thresholds. The PRS was derived using an algorithm involving weighted odds ratios of 29 PCa-associated single nucleotide polymorphisms previously identified. In the PRS adapted model, screening would not be performed in below average risk men. The PSA cutoff for biopsy for the models was determined using a biopsy detection rate of 40% for overall PCa . All models had annual screening events except PRS average risk patients who were screened every 3 years.Results 3986 PCPT participants who were in the placebo arm and had genetic data were included in the analysis: 1316 (33.0%) <60, 2140 (53.7%) 60-69, and 530 (13.3%) >70 years old at study entry. Overall and age stratified results are shown in the table. Amongst all the different models with the different age strata, the PRS risk adapted model was the most efficient, with fewest screening events and largest proportion of cancers detected. The efficiency was greatest in younger men, compared to UPS there were 5,356 fewer screening events, while capturing 13% more high grade tumors, and declines with age. Even so, in men >70, the PRS risk adapted model required. half as many screening events to capture a comparable proportion of high grade cancers as the next best model (PSA >1).Conclusions In this unique dataset, a risk adapted screening approach using a PRS was the most efficient model to minimize screening events and maximize the detection of high grade PCa. 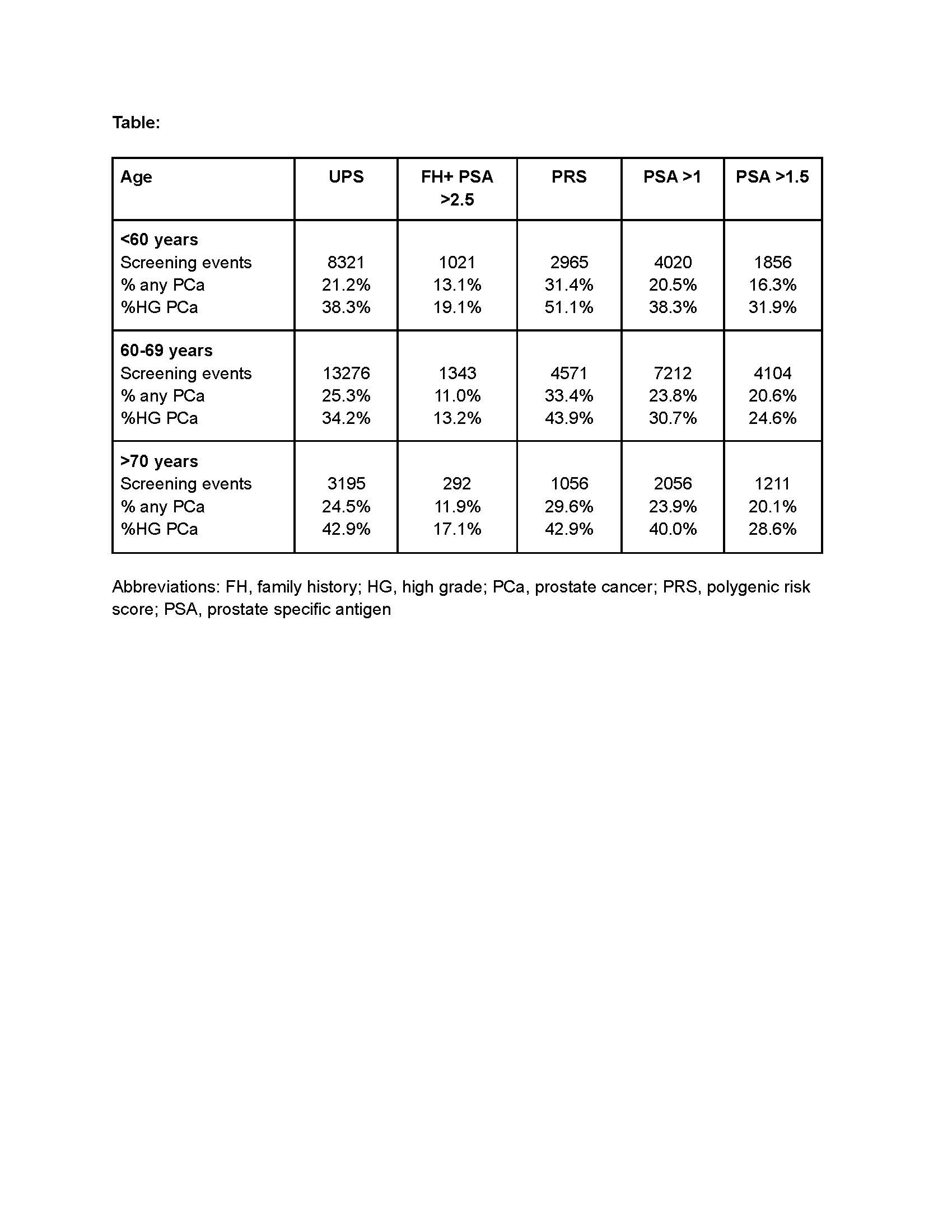
Back to 2022 Abstracts