
Urothelial Cell Carcinoma of the Bladder in Pediatric Patients: A Systematic Review of Case Reports & Case Series
Michael E. Rezaee, MD, MPH1, Charlene M. Dunaway, PhD2, Michael L. Baker, MD1, Frank J. Penna, MD1, David R. Chavez, MD1
1Dartmouth-Hitchcock Medical Center, Lebanon, NH, 2Geisel School of Medicine at Dartmouth, Hanover, NH
Background: Urothelial cell carcinoma (UCC) of the bladder is exceedingly rare in pediatric patients. Limited data is available to guide management in this population.
Methods: We systematically searched MEDLINE, Cochrane Library and Google Scholar (through February 2019) for case reports and series to summarize data regarding presentation, evaluation, management, and follow-up for patients less than or equal to 18 years diagnosed with UCC of the bladder. Patient-level data was abstracted and logistic regression was used to identify factors associated with a combined outcome of recurrence-or-death.
Results: One hundred and two articles describing 243 patients from 26 countries met criteria. Average age was 12.5 years, 32.6% were female, 15.3% had medical comorbidities, and 13.2% had known risk factors for bladder cancer. Initial management was transurethral resection in 95.5% of patients, 12.1% required secondary intervention. Tumor subtype was papillary in 98.3%, 3.3% were muscle invasive, 93.4% were low-grade; the majority of patients were stage TaN0M0 (88.2%). Mean time to recurrence-or-death was 8.6 months (SD 7.6) for 10.7%. Mean disease free follow-up without recurrence-or-death was 56.9 months (SD 54.2) for 89.3%. Patients with comorbidities, risk factors or family history (OR: 2.4, 95% CI: 1.02-5.58) or with greater than TaN0M0 disease (OR: 6.6, 95% CI; 2.64-15.81) had significantly greater adjusted odds of recurrence-or-death after initial treatment.
Conclusion: Based on pooled results, low-grade and stage UCC of the bladder in pediatric patients should likely be systematically monitored with renal/bladder ultrasound, urine analysis and cystoscopy for at least 3 years. Less aggressive surveillance is likely sufficient after this time period. 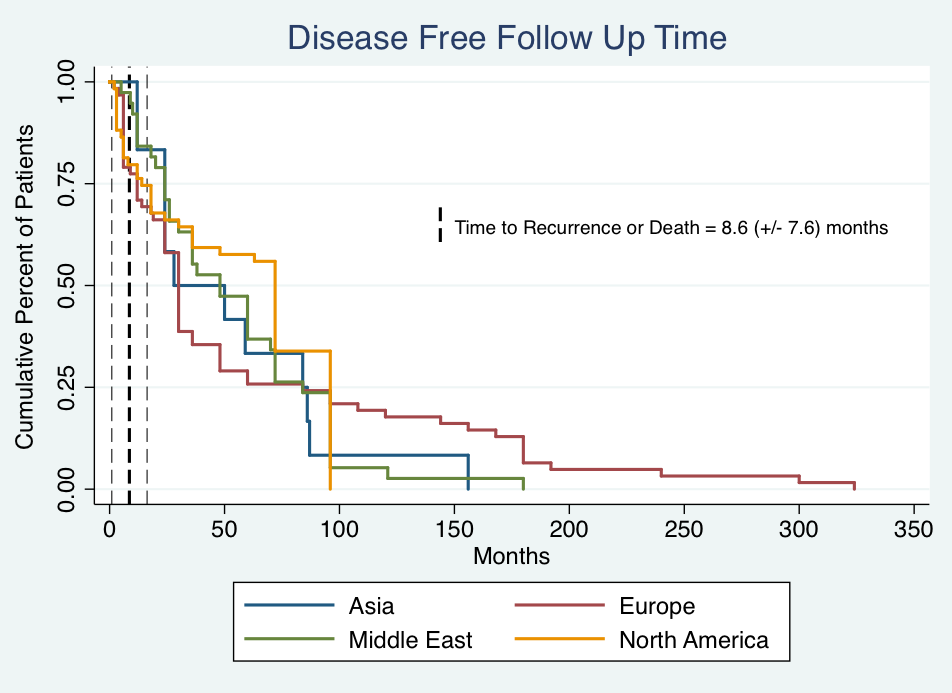
Back to 2019 Abstracts