
The Use of Penile Computed Tomography Cavernosogram (CTC) in the Evaluation of Peyronie's Disease
Jared P. Schober, MD, Sebastian Flacke, MD, Andrew R. McCullough, MD
Lahey Hospital and Medical Center, Burlington, MA
Introduction:
The evaluation of Peyronie’s Disease (PD) relies on patient history and physical exam. The clinical assessment of plaque size and location on exam is qualitative, is observer dependent and has been shown to be unreliable. Current AUA guidelines recommend an office intracorporal penile injection with or without penile color doppler ultrasound. Advanced imaging techniques play a limited role. Intralesional collagenase is the only FDA-approved medical treatment for PD. The benefit of this therapy is highly dependent upon pre-treatment evaluation and appropriate patient selection. Therapeutic benefit has been disappointing. Recent studies have demonstrated the utility for Computed Tomography Cavernosography (CTC) in the evaluation of penile anatomy and erectile dysfunction. Its use in the anatomic evaluation of PD has not been investigated or reported.
Materials & Methods:
Men with documented PD underwent 3D CTC with concurrent intra-cavernosal injection (ICI). Patients were placed in the Philips IQon Spectral CT scanner and an injection of Trimix (papaverine 30 mg/cc, phentolamine 2 mg/cc, prostaglandin 20 mcg/cc) in the proximal base of the penis. The medication dose was determined by pre-existing erectile function. The dose was repeated until a 3 out of 4 erection was achieved (adequate for penetration) or the maximum dose (1cc) had been administered. A 20-gauge angio-catheter was inserted into the left subcoronal corpora after injection of lidocaine for local analgesia. The penis was then manually inflated using a 50% mixture of iodinated contrast solution until maximum erection was achieved. 3D CT imaging was then obtained. A reversal dose of phenylephrine was administered if necessary, the catheter was removed, and a compressive dressing was placed. Images were processed using Philips software v4.7.5.43524.
Results:
The procedure was uniformly well tolerated. Plaque size and location were underestimated by clinical assessment when compared to CTC. Extensive cavernosal disease exceeding previous clinical assessment was frequently identified. Corporal disease was identified in locations inaccessible on physical exam. Precise measurement of the penile angulation in multiple planes was possible through three-dimensional software manipulation of the images. CTC revealed extensive fibrosis and/or atrophy of the underlying corpora cavernosa, identifying patients unlikely to respond to localized collagenase. In these cases, advanced imaging offered benefit in the process of patient counseling and therapeutic decision-making.
Conclusions:
CTC is a valuable tool in the evaluation of Peyronie’s disease. CTC imaging provided enhanced pretreatment assessment of the location, size, and clinically unrecognized severity of disease. The procedure was well tolerated and demonstrated utility in clinical decision-making regarding disease management and patient education. Further prospective studies are needed to determine the role of CTC in the diagnosis and treatment of PD. 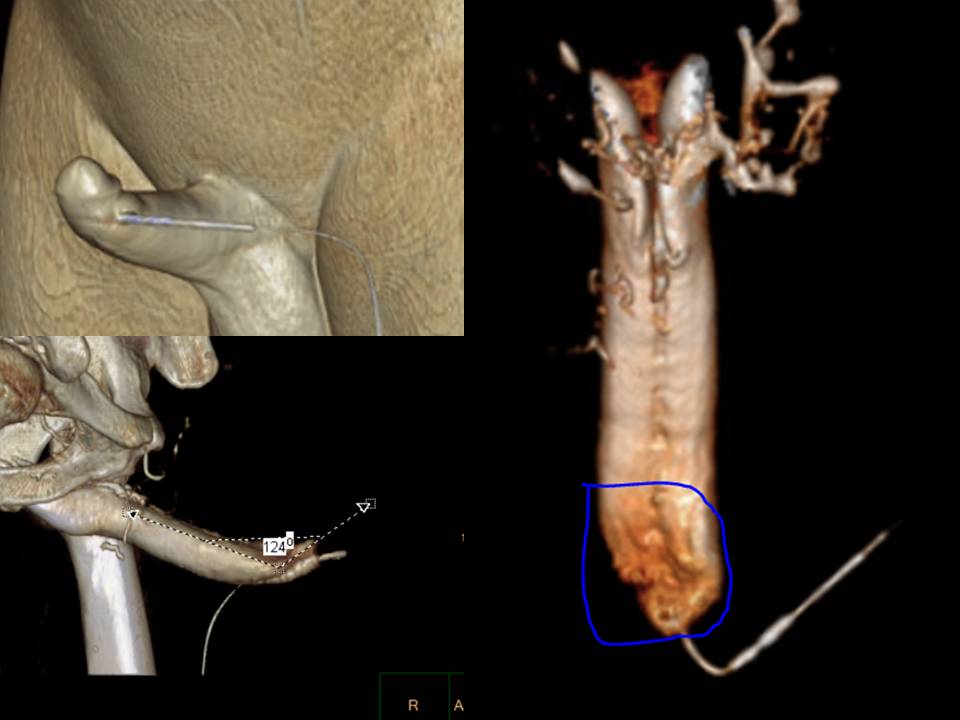

Back to 2019 Abstracts