
Impact of Tumor, Treatment and Access on Outcomes in Bladder Cancer: Can Equal Access Overcome Race-based Differences in Survival?
Alexander P. Cole, MD1; Sean A. Fletcher, BS1; Marieke Krimphove, MD2; Brandon A. Mahal, MD1; Paul L. Nguyen, MD1; Stuart R. Lipsitz, ScD1; Mark A. Preston, MD, MPH1; Adam S. Kibel, MD1; Quoc-Dien Trinh, MD1
1Brigham & Women's Hospital, Boston, MA; 2University of Frankfurt, Frankfurt Main, Germany
BACKGROUND: As with many cancers, there are well-known race-based differences in bladder cancer outcomes, however the optimum strategies to reduce these disparities are not known. We therefore designed a study to assess the relative contribution of tumor, treatment and access-related factors on race-based differences in survival for men and women with bladder cancer.
METHODS: We performed a retrospective, registry based observational study within the National Cancer Database from 2004-2015. Participants included men and women, aged 18 or older, of Black or White race diagnosed with clinically localized or locally advanced muscle invasive bladder cancer. The main outcome was patient race. Using a previously described approach, we assessed the impact of tumor, access and treatment related factors on racial differences in overall survival by fitting propensity score models to which we sequentially added (A) demographics and comorbidities (B) tumor characteristics (C) treatment variables and (D) access to care related variables. We calculated the relative hazard of death of Black and White patients after each weighting procedure. The change in excess mortality was used to infer the contribution of that set of variables on the excess risk of mortality.
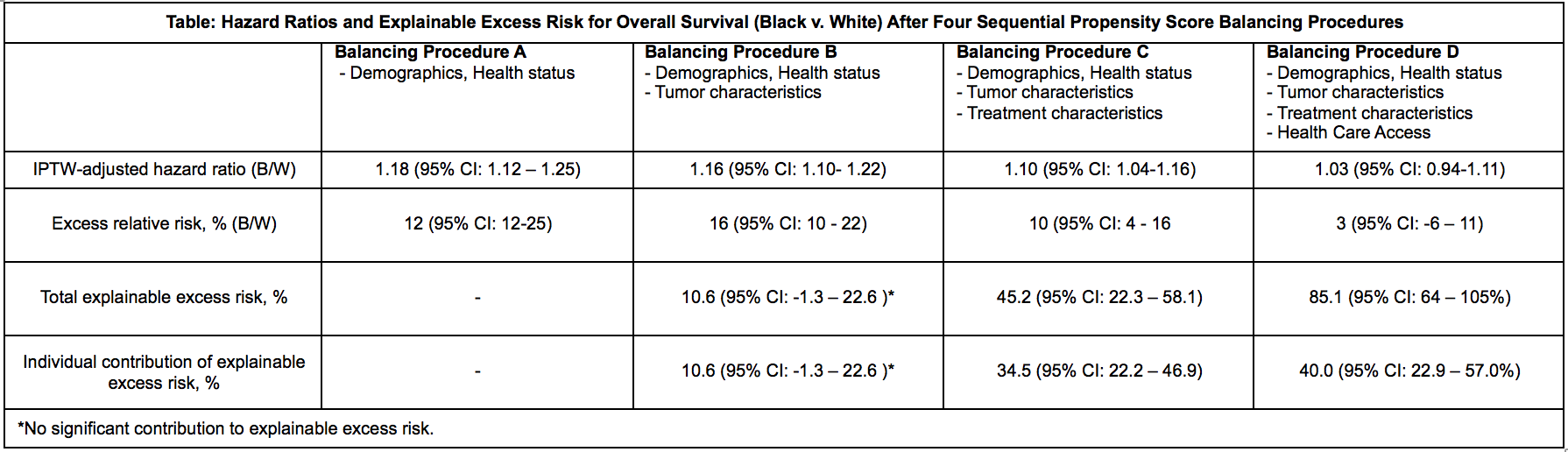
RESULTS: We identified 44,577 patients with clinically localized invasive bladder cancer of Black or White race. The median follow up was 77 months. After balancing for demographics and comorbidities, Black race was associated with a significant adverse effect on overall survival (hazard ratio 1.18, 95% CI 1.12 - 1.25; p < 0.001). After weighting by tumor characteristics, the excess relative risk was reduced from 18% to 16%, and after adding treatment this was reduced to 10%. After adding access variables, the difference in survival was not significant. Overall, access-related variables explained 40% (95% CI 22.9-57.0%) of the excess risk of death among Black patients, followed by treatment factors which explained 34.5% (95% CI 22.2 - 46.9). The individual contribution of biological tumor characteristics was not statistically significant (See Table).
CONCLUSIONS: There are persistent racial differences in overall survival for bladder cancer, which are largely explained by disparities in access to care, and to a lesser extent by disparities in treatment. Black-white differences in assessed tumor biologic characteristics explained little of the difference in overall survival.
Back to 2018 Program