Back to 2017 Program
Equilibrated Bladder Pressure at End Filling: A Lower and Less Variable Measure than Maximum Detrusor Pressure
Joseph W. McQuaid, MD, Michael P. Kurtz, MD, MPH, Tanya Logvinenko, PhD, Stuart B. Bauer, MD, Caleb P. Nelson, MD, MPH, Carlos R. Estrada, MD.
Boston Children's Hospital, Boston, MA, USA.
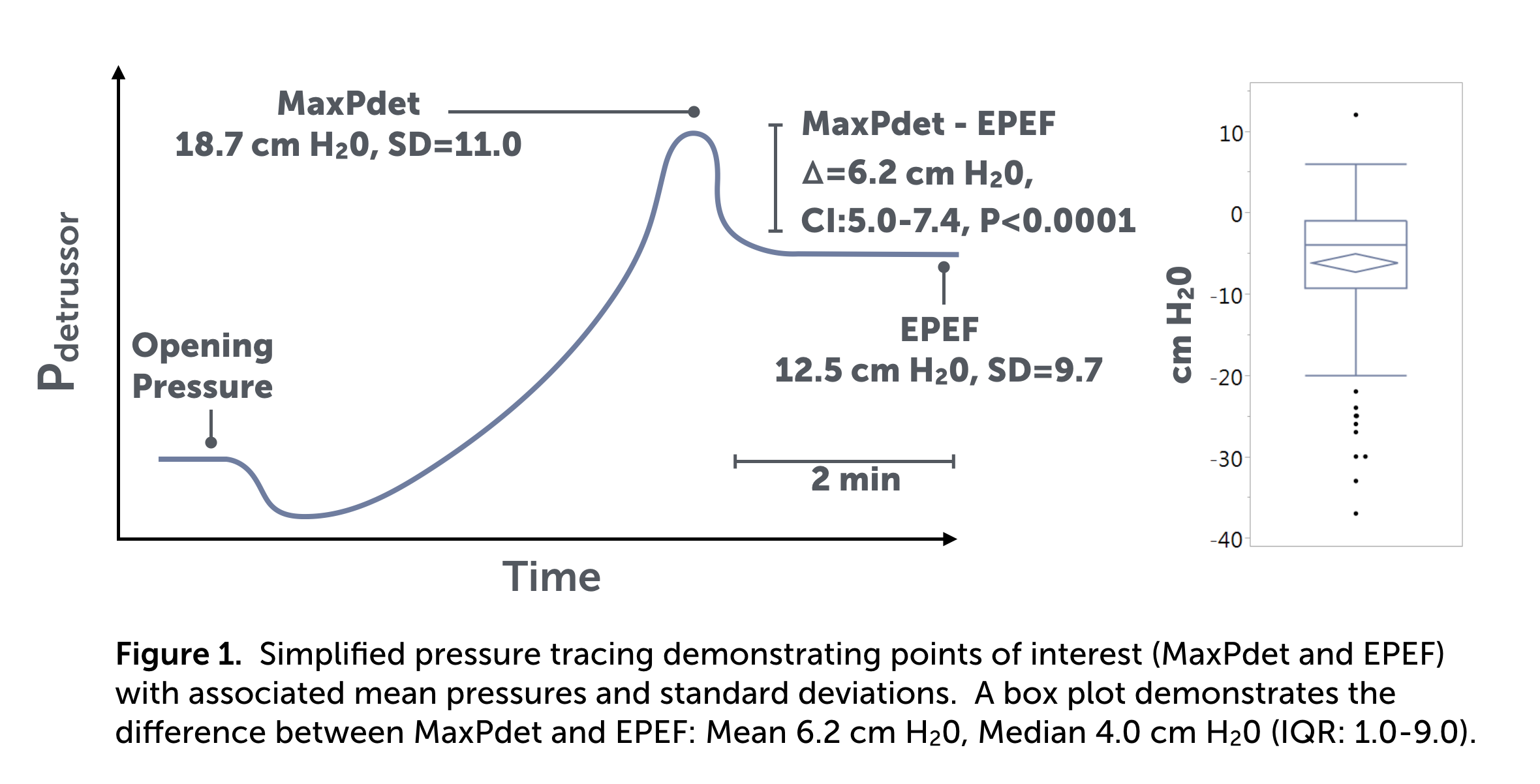
BACKGROUND: Maximum detrusor pressure (MaxPdet), obtained at the end of the filling phase in cystometry, is regarded as an important variable in predicting renal deterioration, but it may be susceptible to artifact induced by the artificial rate of bladder filling. To address this potential artifact, we recorded bladder and intra-abdominal pressures for two minutes after filling had stopped to allow the bladder to reach an equilibrium pressure. The aim of this study was to characterize the equilibrated pressure at end filling (EPEF), a new urodynamic parameter, and to determine its relationship to MaxPdet.
METHODS: We randomly selected 200 initial urodynamic studies performed in children >= 6 years old between 1/2015 and 1/2016, excluding those lacking a recorded EPEF and MaxPdet. The remaining studies (n=181) were reviewed for parameters, MaxPdet and EPEF. The difference between MaxPdet and EPEF was evaluated using the paired t-test, and their variances were then compared with the Pitman-Morgan test. Thereafter, a subset analysis evaluating the effect of anticholinergic or beta agonist usage was completed using the paired t-test.
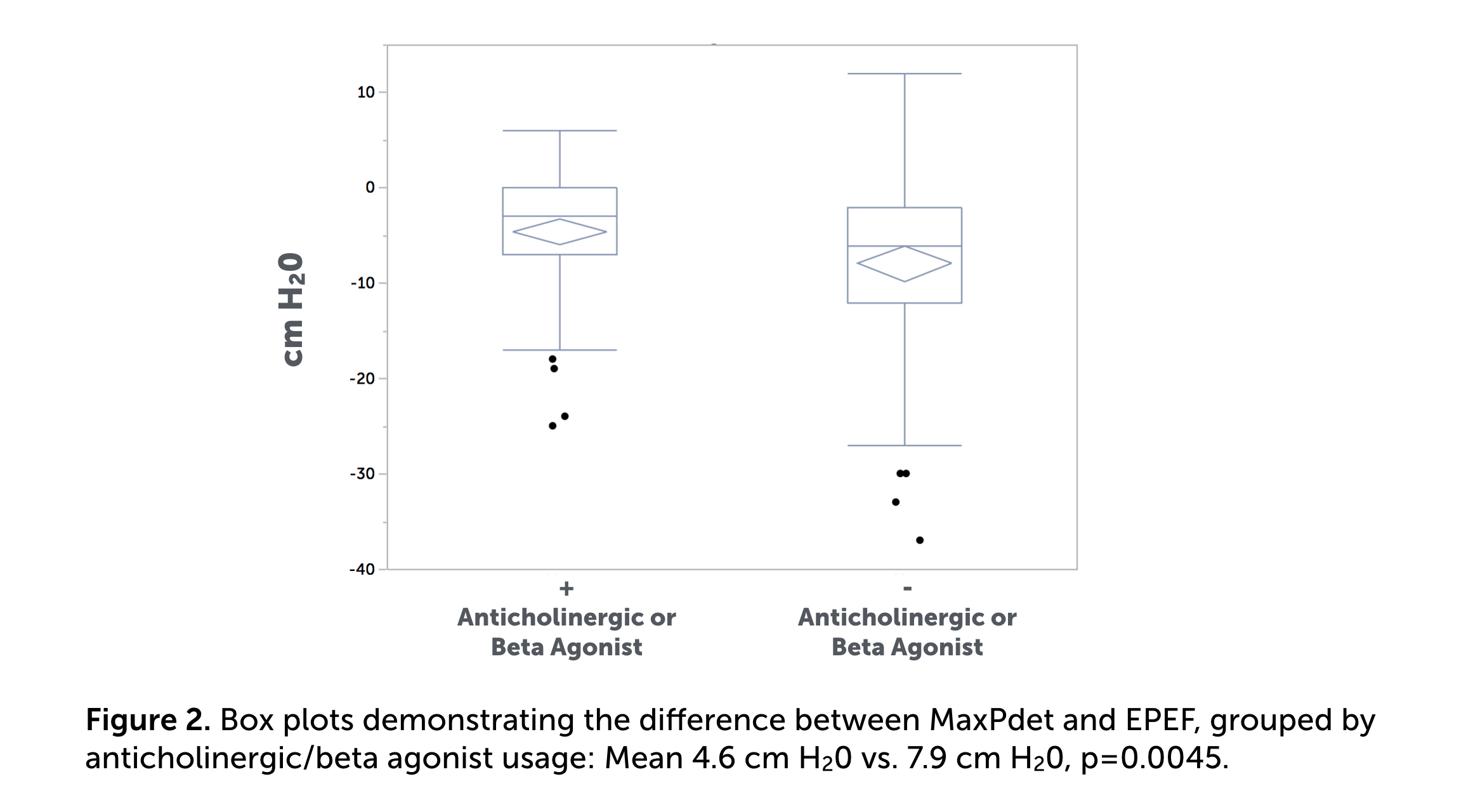
RESULTS: The study included 181 patients (104 females:77 males). Median age = 13.1 years (IQR:9.4-17.0). The three most common indications for study involved: spina bifida (n=85, [47.0%]), incontinence (n=51, [28.2%]), and tethered cord (n=41, [22.7%]), with some children having >1 indication. 92 (50.8%) were taking either an anticholinergic or beta agonist at the time. Of 181 studies, EPEF was lower on average than MaxPdet by 6.2 cm H20 (95%CI:5.0-7.4, p<0.0001). The standard deviation of EPEF was smaller than that for MaxPdet (9.7 vs. 11.0, p=0.0123) (Figure 1). An in-depth analysis of 35 children (19.3%) who did not leak between MaxPdet and EPEF measurements revealed that, on average, EPEF was < MaxPdet by 4.0 cm H20 (95%CI:1.8-6.2, p=0.0007). When analyzing children on bladder modulating medication, the difference between MaxPdet and EPEF was smaller for those taking either an anticholinergic or beta agonist than for those on no medicines (4.6 vs. 7.9 cm H20, p=0.0045) (Figure 2).
CONCLUSIONS: Allowing for equilibration after maximum bladder filling results in a significant average decrease in detrusor pressure by 6.2 cm H20. The EPEF demonstrates a smaller variance and may more accurately reflect the maximal pressure exhibited by the bladder under physiologic conditions. Given the difference between MaxPdet and EPEF is smaller in children taking either an anticholinergic or beta agonist, we hypothesize these medications may provide a protective benefit against pressure artifacts introduced by standard fill (10% of expected capacity/min) cystometry.
Back to 2017 Program
|
|
|
|



