Back to 2017 Program
Survival Analysis of Cytoreductive Nephrectomy in the Elderly
Ariel K. Fredrick, MD, Kristian D. Stensland, MD, Jared Schober, MD, Marc D. Calabrese, MD, David Canes, MD, Alireza Moinzadeh, MD.
Lahey Hospital and Medical Center, Burlington, MA, USA.
BACKGROUND: Renal cell carcinoma has shown to be one of the few cancers responsive to resection of the primary lesion in the setting of metastatic disease. Cytoreductive nephrectomy has been previously evaluated in the population as a whole, but the aging of the population and increasing health status in older patients necessitates evaluation in an explicit cohort. Using the National Cancer Database, the effect of cytoreductive nephrectomy was explored specifically in the elderly population.
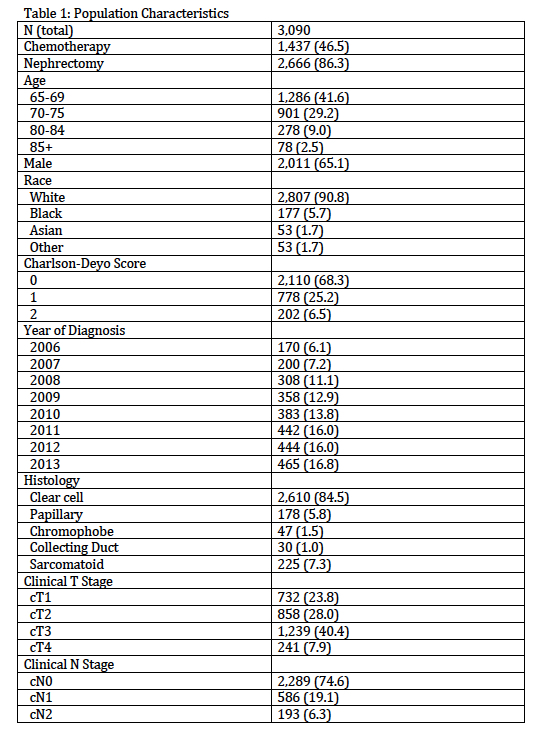
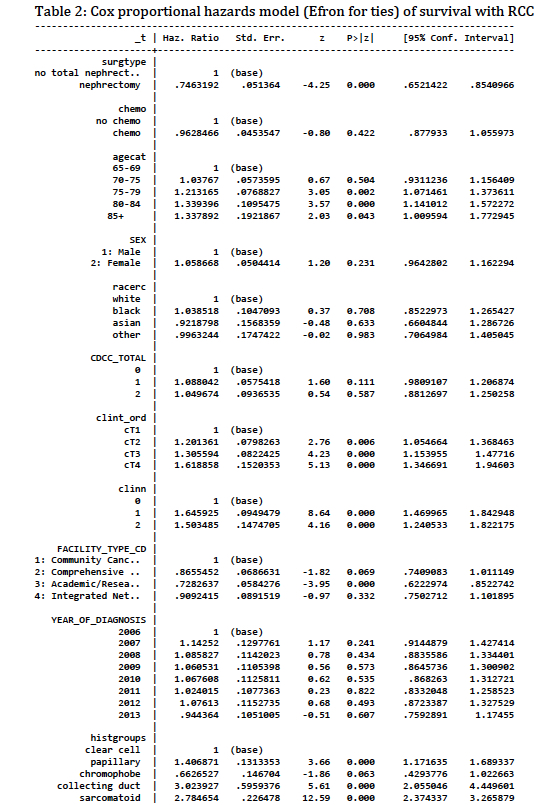
METHODS: The National Cancer Database was used to identify patients >=65 years of age with renal cell carcinoma (clear cell, papillary, chromophobe, collecting duct or sarcomatoid histology) presenting with clinical M1 disease. Analysis was limited to patients with known clinical T1-4 and known clinical N0-2 status. Chemotherapy use, including targeted therapies, was defined as receipt of any (single or multiagent) chemotherapy. The study was limited to years 2006-2013 to reflect the “targeted therapy” era of RCC management. Included patient characteristics were compared using chi-squared or t-tests as appropriate. Cox proportional hazards modeling was used to assess survival. All analyses were performed in Stata.
RESULTS: The majority (86.3%) of adults over 65 with metastatic RCC received cytoreductive nephrectomy, while less than half (46.5%) received chemotherapy including targeted therapy (Table 1). On multivariate Cox regression analysis controlling for other factors, cytoreductive nephrectomy was associated with a hazard ratio of 0.746 [95%CI 0.65-0.85, p<0.001], corresponding to a roughly 25% risk reduction of death from any cause secondary to surgery (Table 2). Receipt of chemotherapy was not associated with significant risk reduction. Increasing age was associated with greater risk of death, with patients in the 75-79, 80-84, and 85+ age groups demonstrating risk increases of 21-34% (Table 2). Other characteristics independently associated with risk of death included papillary, collecting duct or sarcomatoid histology; higher clinical T or N stage; or treatment at a non-academic center (Table 2).
CONCLUSIONS:
Performance of cytoreductive nephrectomy is significantly independently associated with survival in patients over 65 years of age. Patients in this population should be counseled on the benefits of cytoreductive nephrectomy, but care should be taken to evaluate surgical risk in the setting of performance status in addition to clinical and oncologic factors.
Back to 2017 Program
|
|
|
|



