Back to 2017 Program
PSA screening at the intersection of Politics and Policy
Jesse D. Sammon, DO1, Emily C. Serell, MS1, Malte Vetterlein, MD2, Patrick Karabon, MS3, Gregory J. Mills, BA1, Moritz H. Hansen, MD1, Mani Menon, MD3, Quoc Dien-Trinh, MD2, Firas Abdollah, MD3.
1Center for Outcomes Research and Evaluation, Portland, ME, USA, 2Brigham and Women's Hospital, Boston, MA, USA, 3Henry Ford Health System, Detroit, MI, USA.
BACKGROUND: The implementation of health care policy in the U.S. may be impacted by conflicting political philosophies. A ″conservative″ view of health care emphasizes an individual′s right to self-determination, while a ″liberal″ view holds that government can effectively utilize strategies to balance the needs of the community with those of an individual. Federal screening guidelines promoting population health may be perceived to conflict with conservative values. The aim of this study was to assess the inter-relationship of a states percentage of ″conservative″ men and the impact that the 2012 USPSTF recommendation against PSA-based prostate cancer (PCa) screening on screening probability.
METHODS: Data from the 2012 and 2014 Behavioral Risk Factor Surveillance System was used to identify asymptomatic men (age ≥ 50) without PCa who reported PSA screening in the past 12 months. Odds ratios were determined by multivariate logistic regression analysis, adjusting for age, race, education, income, insurance, healthcare access, and marital status. The change in PSA screening rates were assessed as a function of the percentage of adults in a state describing themselves as ″conservative″ or ″very conservative″ in Gallup U.S. Daily (accessed 4/4/16).
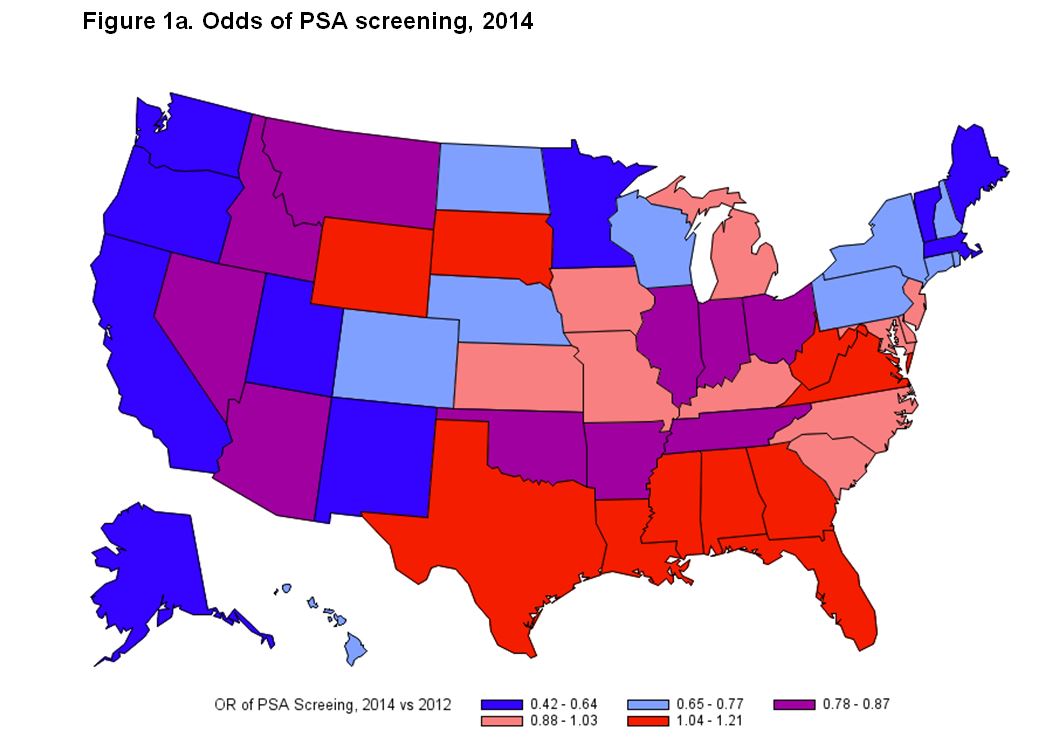
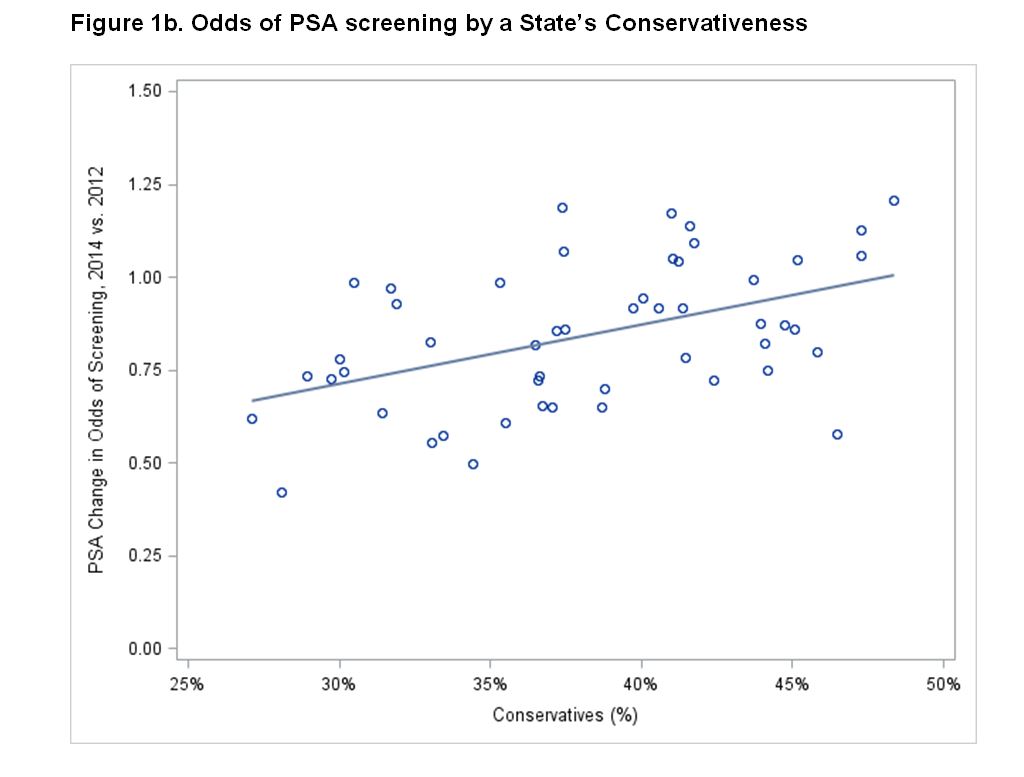
RESULTS: Among 222,475 survey respondents, the prevalence of PSA screening decreased between 2012 and 2014 (OR=0.87, p<0.001; Fig 1a). In the most conservative states (upper tertile of self-described conservatives) screening prevalence was unchanged (OR=0.92, CI 0.84-1.00), and in the least conservative states (lowest tertile) there was a significant decline (OR=0.72, CI 0.64-0.81; Fig 1b). Up to 22% of the variation in PSA screening rates may be ascribed to a state′s dominant political leaning (coefficient of determination=0.22), a moderate and significant correlation (ρ= 0.47, P<0.001).
CONCLUSIONS: The changes in PSA screening rates appear to reflect the political divide in the U.S. Despite the 2012 USPSTF guideline and subsequent overall decrease in PSA screening, there was no decline in PSA screening in the most conservative states. This is a hypothesis-generating finding, as it is predicated on observational data that may be affected by other factors. Nonetheless, this finding suggests that a state′s dominant political ideology influences the implementation of federal health care screening policy.
Back to 2017 Program
|
|
|
|
|



