Back to 2017 Program
USPSTF Fallout: Is Disease Burden at Diagnosis of Metastatic Disease Rising?
Jared P. Schober, MD, Kristian D. Stensland, MD, Alireza Moinzadeh, MD, David Canes, MD.
Lahey Hospital and Medical Center, Burlington, MA, USA.
Background:
The impact of the USPSTF on PSA screening behavior would not be expected to impact metastatic disease rates (mPCa) for several years. However a delay in diagnosis for men with prevalent mPCa might be measurable in the near term. Since PSA is a rough surrogate for disease burden, we sought to determine if the PSA at the time of diagnosis of mPCa is rising in the National Cancer Database (NCDB).
Methods:
The NCDB was used to examine PCa diagnoses from 2004-2014. To minimize reporting bias, only hospitals contributing at least one case per year for the entire decade were included. Cases with cM1 disease were defined as metastatic. PSA at initial cancer diagnosis was divided into 4 groups: 0.2-3.9, 4.0-10.0, 10.1-20, and >20 ng/ml. The ratio of mPCa compared to total PCa diagnoses were compared for each year. Descriptive statistics and a multivariate logistic regression were performed in Stata.
Results:
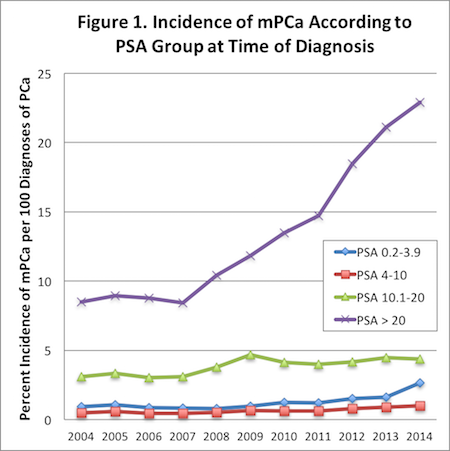
The proportion of mPCa present at initial diagnosis increased over the 10-year period for every PSA group. The most significant proportional increase was observed in patients with PSA >20, from 8.5% (2004) to 22.9% (2014). The most significant rate of increase was observed after 2007 (Figure 1). On multivariate regression, PSA category was independently associated with the presence of metastatic disease at initial diagnosis (p<0.001). The percentage of patients with mPCa at initial diagnosis who had a PSA >20 was 47% in 2004 vs. 72% in 2014. Patients with a PSA <4 had a higher rate of metastatic disease at diagnosis when compared to the PSA 4-10 group. Those with PSA <4 experienced a proportional increase in mPCa from 0.92% (2004) to 2.65% (2014).
Conclusion:
As expected, the presence of mPCa increases with increasing PSA, but the new finding of disproportionately more men with PSA >20 at diagnosis of mPCa in recent years is notable. We hypothesize this may represent higher disease burden at diagnosis as a near term result of USPSTF recommendations. Secondary observation of a proportionate increase in overall mPCa in the NCDB must be interpreted with caution, given that this is a registry rather than a population based dataset. Further studies are needed to elucidate if these trends equate to a greater burden of disease at diagnosis of mPCa, and whether screening behavior is causative.
Back to 2017 Program
|
|
|
|



