Back to 2025 Abstracts
Implementation of Strict Pre-operative Selection Criteria for the Male Urethral Sling Results in Comparable Treatment Outcomes to the Artificial Urinary Sphincter
Philip Olson, MD1, Avery Pollicita, BS
2, Ilene Staff, PhD
2, Kevin Pinto, BS
3, Tara McLaughlin Proto, PhD
3, Laura Olivo Valentin, BS
3, Joseph Tortora, MS
3, Richard Kershen, MD
3.
1UConn Health, Farmington, CT, USA,
2Hartford Hospital, Hartford, CT, USA,
3Hartford Healthcare, Hartford, CT, USA.
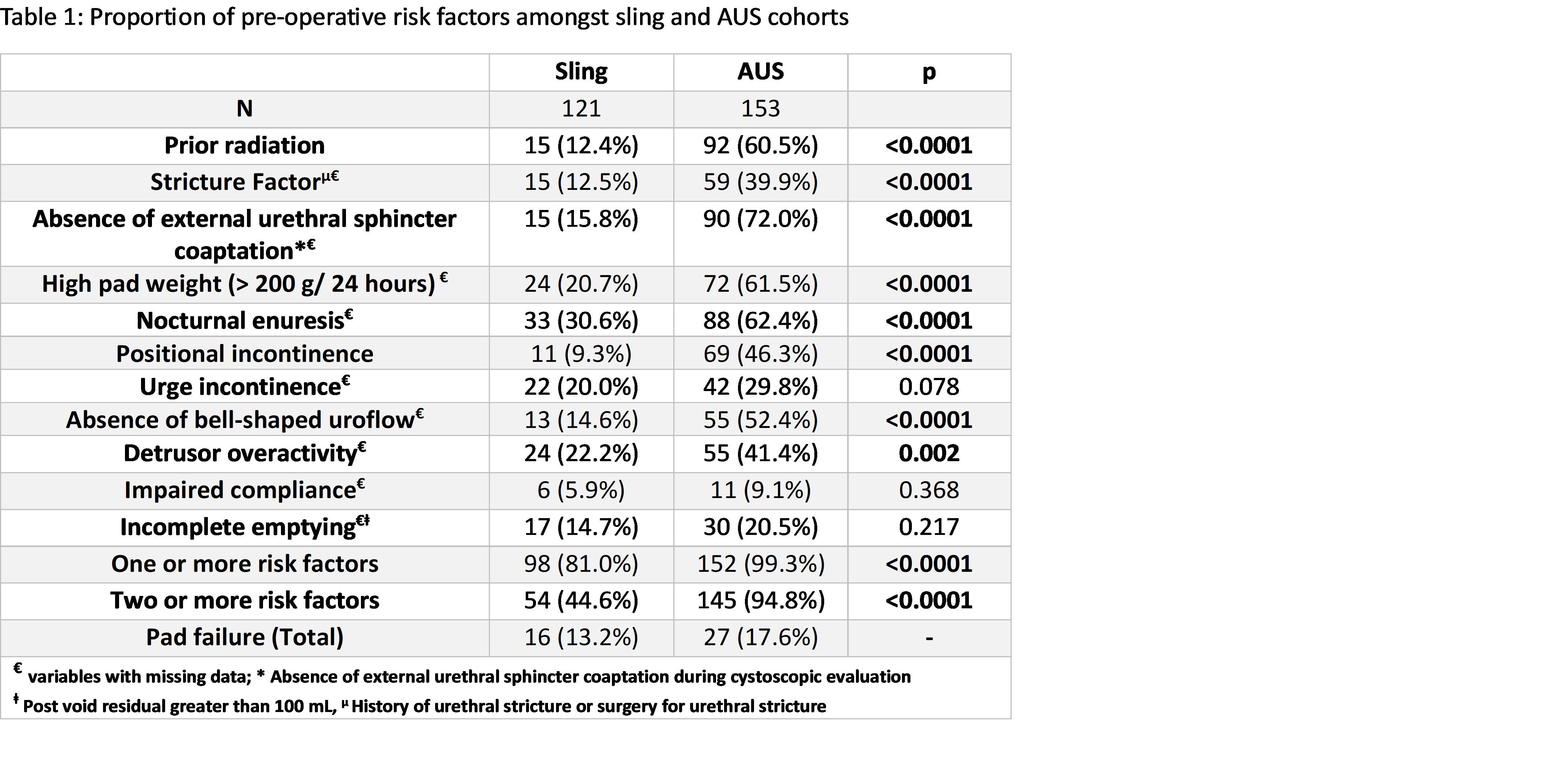
BACKGROUND: Though treatment success for stress incontinence is historically higher using an artificial urinary sphincter (AUS), patients prefer the male sling (MS). Studies have sought to identify pre-operative risk factors (RF) that increase sling failure. We incorporated 11 RF into our preoperative selection process, expecting that their use would produce continence outcomes comparable to the AUS. To test the utility of this selection process, we analyzed the incidence of RFs and pad failure for men in each group.
METHODS: We retrospectively identified men who underwent either MS or AUS placement by one surgeon between January 2012-January 2024. RF rates were compared between MS and AUS. Failure was defined as postoperative usage of >1 pad per day. To avoid any confounding from our pre-operative selection, we compared our MS failure rates to the published AUS failure rate of 21%.
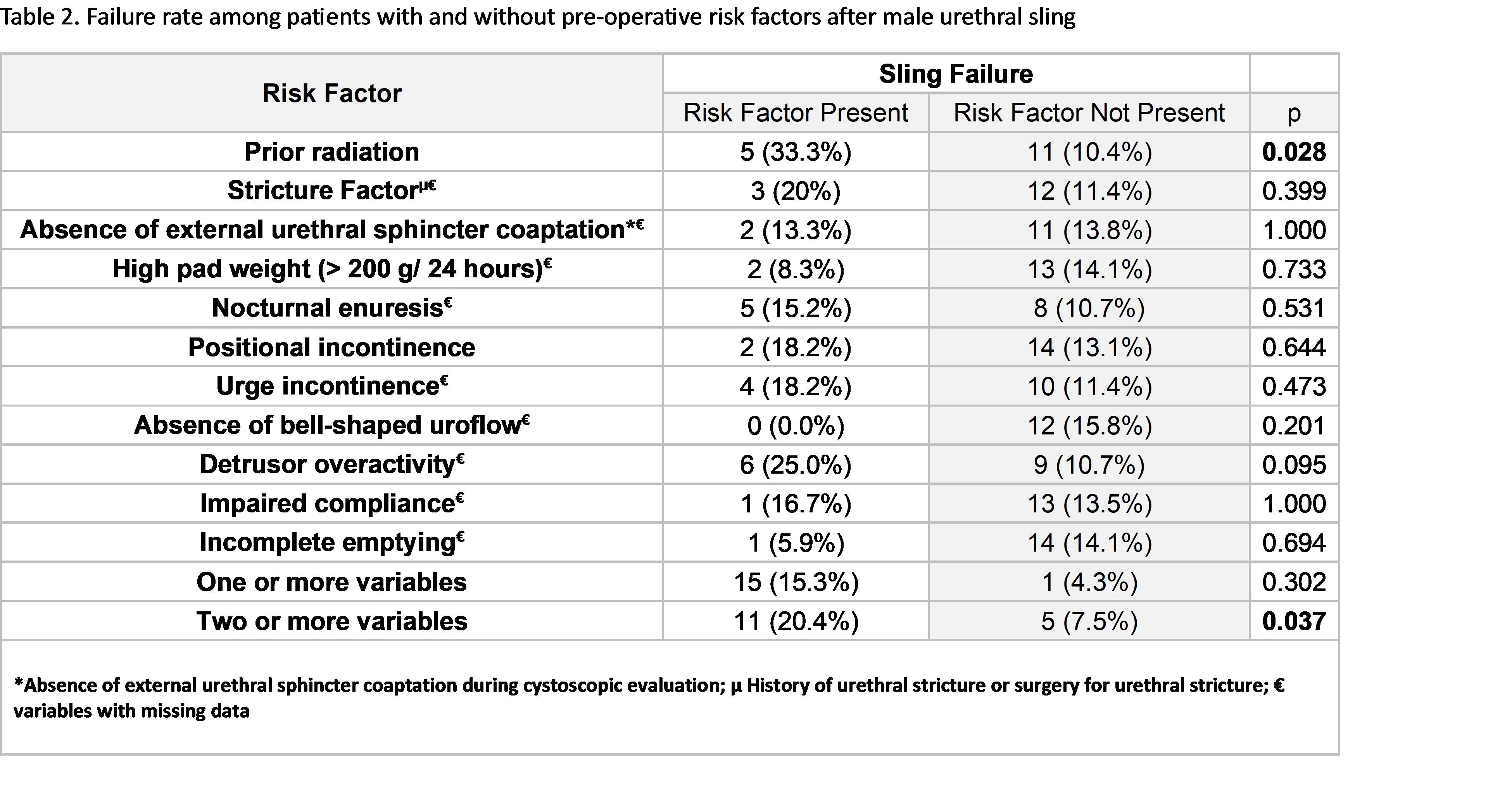
RESULTS: Significant group differences were noted in rates of 8/11 RF (Table 1). 105 patients (87%) and 126 patients (82%) experienced �pad success� for MS and AUS, respectively, with no significant difference. MS failure rate was significantly lower than the published AUS failure rate [13 % vs. 21 % (p= 0.035). The MS failure rate for those with ≥2 RF was significantly higher than those with ≤1 RF [11 (20.4%) vs. 5 (7.5%), p= 0.037] (Table 2).
CONCLUSIONS: Our data suggest selection of patients who have fewer RFs for sling failure produces comparable success rates to the AUS, and in appropriately selected patients MS represents the gold standard in their care.
Back to 2025 Abstracts


