Back to 2025 Abstracts
Pre-Treatment Predictors of Pathological Failure at One Year Following Focal Therapy for Localized Prostate Cancer
Nethusan Sivanesan, BS, Gabriela M. Diaz, MD, Xiwen Zhao, MPH, Peter S. Palencia, BS, Wei S. Tan, MD, PhD, Preston C. Sprenkle, MD.
Yale School of Medicine, New Haven, NC, USA.
BACKGROUND: Predictors of pathological failure following focal therapy (FT) for localized prostate cancer remains poorly characterized. This study evaluates pre-treatment clinical and pathological factors associated with pathological failure at one-year post-ablation biopsy.
METHODS: A retrospective review of an IRB-approved institutional database identified patients who underwent subtotal FT as primary treatment. Clinical parameters, including demographics, MRI findings, biopsy results, PSA metrics, and genomic scores, were analyzed. Pathological failure was defined as recurrence of Gleason Grade (GG) ≥2 prostate cancer at mandatory one-year biopsy. Fisher�s exact test and Wilcoxon rank-sum test were used to evaluate associations between pre-treatment factors and pathological failure.
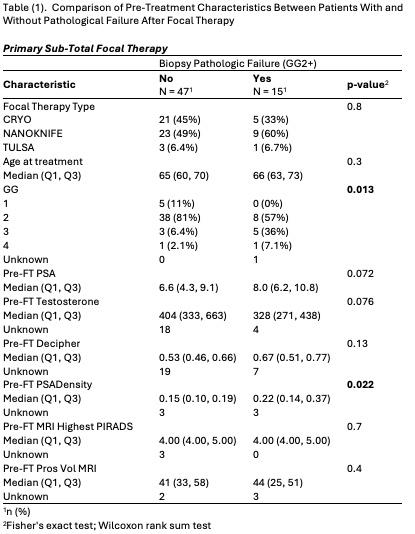
RESULTS: Among 62 patients, 15 (24.1%) demonstrated pathological failure, while 47 (75.9%) had no recurrence. Patients with pathological failure had significantly higher pre-ablation Gleason Grade (p = 0.013) and pre-ablation PSA density (PSAD) (p = 0.022) compared to those without recurrence. Other pre-treatment factors, including PSA level, testosterone, Decipher genomic classifier score, highest MRI findings, type of FT (cryotherapy vs NanoKnife vs TULSA), and patient age were not significantly associated with recurrence (Table 1).
CONCLUSIONS:Higher pre-ablation GG and PSAD were significantly associated with pathological failure at one year following FT. These findings suggest that baseline Gleason score and PSA density may help stratify patients at higher risk for recurrence post-treatment.
Back to 2025 Abstracts


