Back to 2025 Abstracts
Can Anatomical Measurements on Preoperative Pelvic Magnetic Resonance Imaging Predict Postoperative Urinary Incontinence After Holmium Laser Enucleation of the Prostate?
Shayan Smani, BS1, Amir I. Khan, MD
2, Ankur U. Choksi, MD
1, Benjamin H. Press, MD
1, Syed N. Rahman, MD
1, Christopher S. Hayden, MD
1, Mursal Gardezi, MD
1, Michael Jalfon, MD
1, Jason J. Lee, MD
1, Preston C. Sprenkle, MD
1, Daniel S. Kellner, MD
1.
1Yale University School of Medicine, New Haven, CT, USA,
2Vanderbilt University School of Medicine, Nashville, TN, USA.
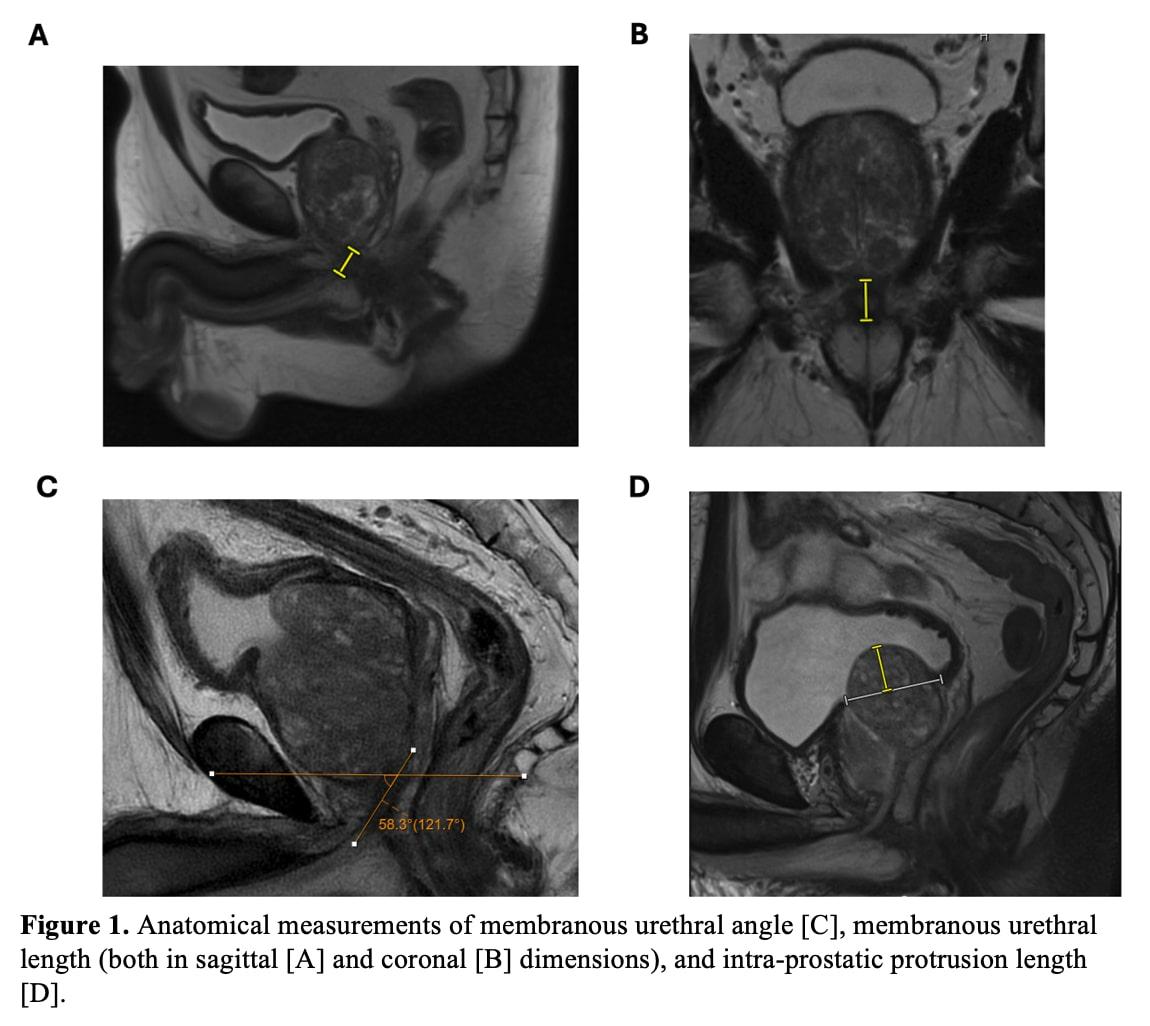
BACKGROUND: Anatomical dimensions of the prostate and membranous urethra are well-established predictors of urinary incontinence following robotic prostatectomy. However, their role in predicting incontinence after holmium laser enucleation of the prostate (HoLEP) remains underexplored. This study evaluated the predictive value of preoperative anatomical measurements, including membranous urethral length (MUL), membranous urethral angle (MUA), levator ani thickness (LAT), and intravesical prostatic protrusion length (IPPL), in assessing early postoperative urinary incontinence following HoLEP.
METHODS: We retrospectively reviewed 122 patients who underwent HoLEP from April 2019 to June 2022 with preoperative MRI. Anatomical features including coronal and sagittal MUL, MUA, LAT, and IPPL were assessed. Urinary incontinence, defined as the use of ≥1 pad per day, was evaluated at 1-, 3-, and 6-months postoperatively. Logistic regression analyses were adjusted for age, BMI, post-void residual, preoperative incontinence, and PSA, and ROC curves were constructed to assess the discriminatory utility of MRI anatomical measurements.
RESULTS: Increasing MUL was significantly associated with reduced incontinence risk at 1 month (coronal MUL: OR, 0.85; 95% CI, 0.75-0.96; P = 0.01; sagittal MUL: OR, 0.89; 95% CI, 0.79-0.99; P = 0.046). No significant associations were found for MUA, LAT, or IPPL. ROC analysis of averaged coronal and sagittal MUL revealed moderate discriminatory power (AUC: 0.644), with a threshold of 14 mm identified via the Youden index. Individuals with an MUL < 14 mm had nearly 4-fold increased odds of incontinence at 1 month (OR 3.835, 95% CI, 1.516-9.703; P = 0.005).
CONCLUSIONS: Preoperative MUL measurement provides a practical, imaging-based method to predict early postoperative incontinence following HoLEP. Incorporating MUL into preoperative evaluations may improve risk stratification, patient counseling, and perioperative management.
Back to 2025 Abstracts


