Back to 2025 Abstracts
Artificial Urinary Sphincters in the setting of Radiation Cystitis: A Cohort Study
Grayden S. Cook, MD, Martin N. Kathrins, MD.
Mass General Brigham, Boston, MA, USA.
BACKGROUND: Radiation cystitis, when coupled with the presence of an artificial urinary sphincter (AUS), can be a challenging scenario to manage. Given the paucity of literature on this patient population, we sought to elucidate the outcomes of our institutional experience in this cohort.
METHODS: Utilizing our institutional research patient data registry from 2010-present for Brigham and Women�s Hospital and Mass General Hospital, we queried to identify patients with an AUS in place during documented diagnosis of radiation cystitis. We further stratified patients by having an acute episode of radiation cystitis which was defined by requiring admission to the hospital for gross hematuria. Chart review was then performed on each patient to accumulate patient characteristics and clinical outcomes data.
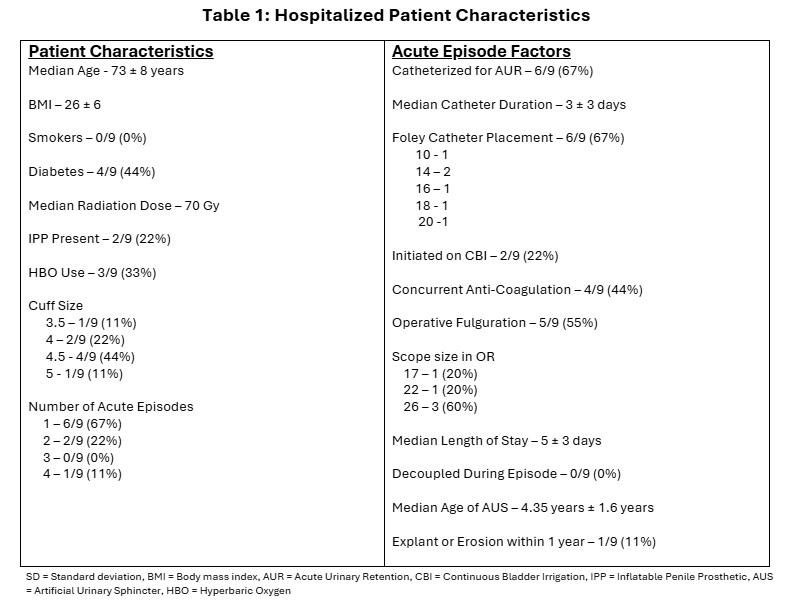
RESULTS: Our query identified 410 patients from 2010 with an AUS, of which 27/410 (6%) patients had an AUS and documented diagnosis of radiation cystitis. Cystoscopic diagnosis of radiation cystitis was seen in 21/27 (78%) of patients compared to 6/27 (22%) with pathologic diagnosis. 9/27 (33%) patients suffered acute episodes of radiation cystitis requiring hospital admission for gross hematuria; of which 6/9 (67%) required catheter placement for acute clot retention. Breakdown of patient characteristics during acute episodes such as catheter size and need for operative intervention including scope size are illustrated in Table 1.
CONCLUSIONS: Our institutional experience demonstrates that the majority of patients presenting with an acute episode of radiation cystitis with an AUS require catheterization and operative intervention for definitive treatment. Reassuringly, only 1/9 (11%) patients experienced AUS erosion or required an explant after an acute episode requiring hospitalization. In our population, serious AUS complications from radiation cystitis were overall uncommon.
Back to 2025 Abstracts


