Back to 2025 Abstracts
Modeling survival outcomes of KEYNOTE-564 with standard of care control arm treatment: A simulation study.
Fady Ghali, MD1, Keervani Kandala, BS
1, Syed N. Rahman, MD
1, Spencer L. James, MD, MPH
2.
1Yale University School of Medicine, New Haven, CT, USA,
2Docere.ai, Seattle, WA, USA.
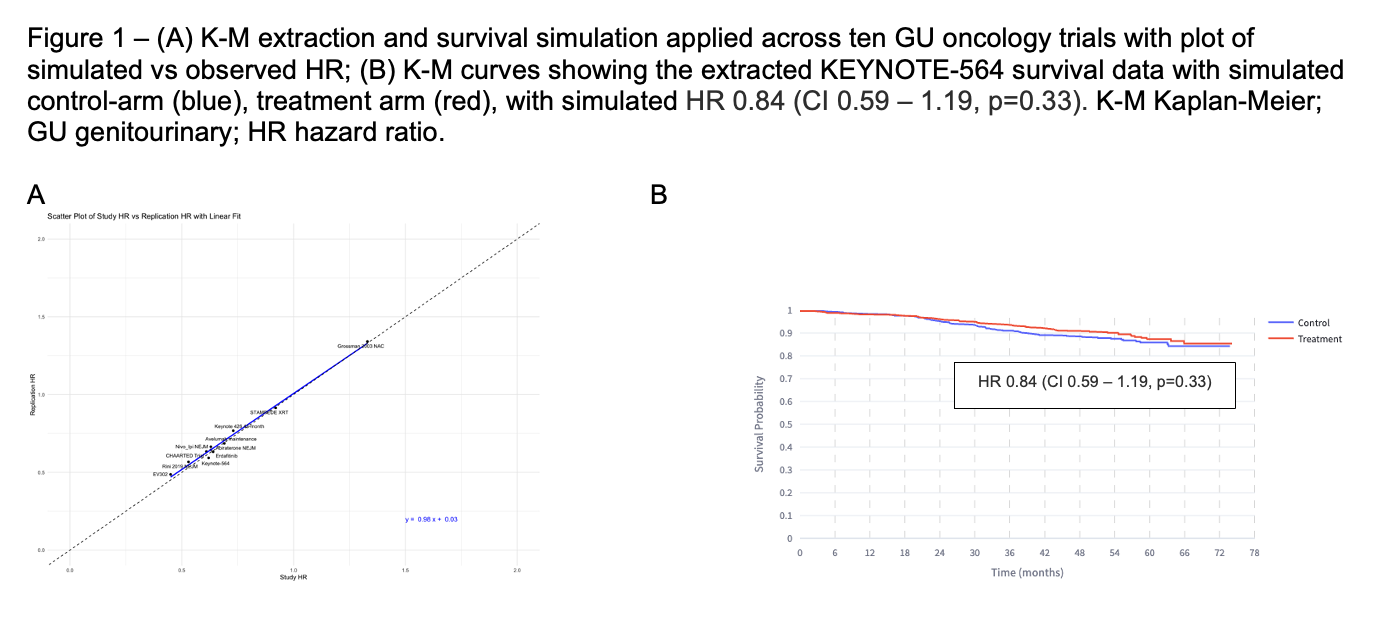
Background: The KEYNOTE-564 study, reporting improved overall survival (OS) with adjuvant checkpoint inhibitor (CPI) in renal cell carcinoma (RCC) suffers from a common challenge: a portion of control-arm received non-standard of care (nSOC) subsequent therapy upon progression, thus underestimating their survival. We sought to simulate KEYNOTE-564 using SOC control-arm to assess adjuvant CPI more accurately.
Methods: Reconstructed individual patient data from Kaplan-Meier curves (K-M) as published in CHECKMATE-214 and KEYNOTE-564 were extracted. Attributable risk between treatment groups within K426 were simulated. We validated both our K-M extraction method as well as our survival estimate method by re-generating survival plots and comparing to the published outcomes across 10 genitourinary (GU) oncology trials. Survival benefit estimates from CHECKMATE-214 were incorporated to KEYNOTE-564 in a weighted fashion - these measures estimate counterfactual OS outcome for the KEYNOT-564 control group using CHECKMATE-214 outcomes to approximate the increase in survival had they received SOC upon progression.
Results: Across 10GU-oncology trials, our methods accurately re-simulated survival estimates compared to observed date(Figure 1A). Within KEYNOTE-564, 54.5%(N = 123) of patients in the control-arm that experienced progression are not reported to have received CPI. We estimate 20-fewer deaths in the control-arm had all patients received dual-CPI upon progression; HR 0.84(CI0.59-1.19,p=0.33)(Figure 1B). On sensitivity analysis, an OS benefit in KEYNOTE-564 is only observed if dual-CPI survival benefit is applied to ≤45%(N=55/123) control-arm progressors.
Conclusions: We validate a method for simulating outcomes under SOC therapy for clinical trials where nSOC treatment limits the interpretation of their conclusions. In a simulation correcting for the nSOC therapy in control-arm of KEYNOTE-564, the reported survival benefit of adjuvant CPI was not seen.
Back to 2025 Abstracts


