Back to 2025 Abstracts
Urologic outcomes following abdominoperineal resection: a multi-institutional analysis
Sami Wilder, MD
1, Anna Saltman, MD, MS
2,
Brielle Barclay-Rochefort, DPT2, Andrew Mizerowski, BA
1, Michael Callegari, MD, MBA
2, Caroline Kreytak, BA
2, Mateo Mora, MD
1, Logan Hubbard, MD
1, Nabeel Shakir, MD
1, Alex Vanni, MD
2, Marcus Jamil, MD
1.
1Henry Ford, Detroit, MI, USA,
2Lahey, Burlington, MA, USA.
BACKGROUND: Abdominoperineal resection (APR) involves removing the distal colon, rectum, and anal sphincter for oncologic and benign conditions. Urinary and sexual dysfunction may occur due to pelvic trauma or neurovascular injury. This study evaluates urologic outcomes, including intraoperative injuries and postoperative dysfunction, following APR at two high-volume tertiary centers.
METHODS:We retrospectively reviewed APR cases from 2013 to 2024 at two tertiary centers. Data on urologic injuries, lower urinary tract symptoms (LUTS), and erectile dysfunction (ED) were collected. Statistical analysis was performed using JMP 18.1.0, with significance set at 0.05.
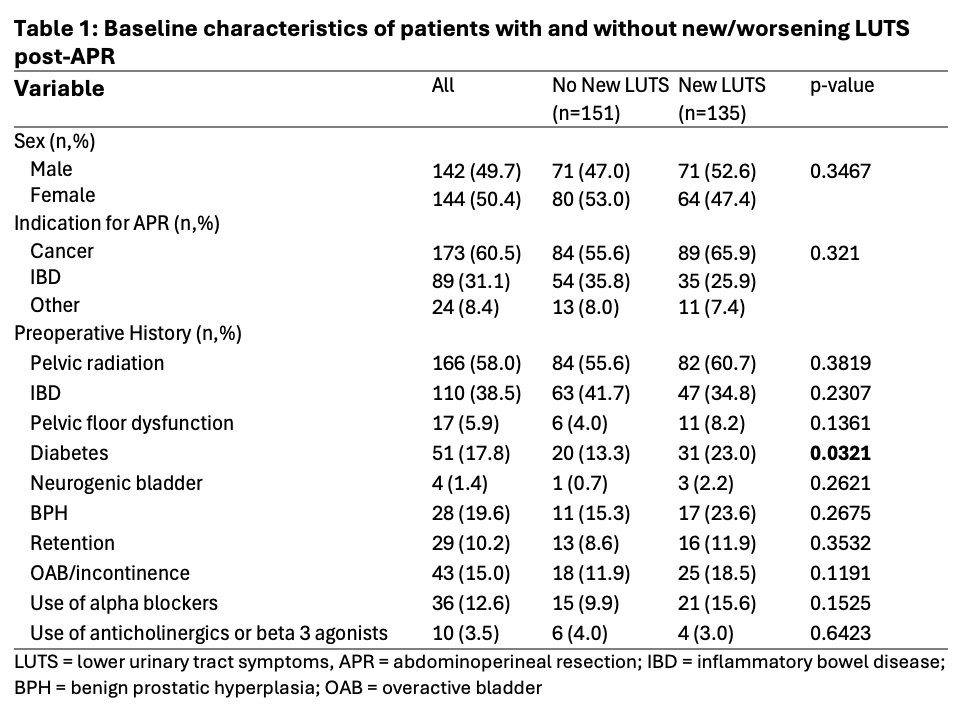
RESULTS:Among 286 patients (142 men, 144 women), mean age was 59.3 years. APR was performed for cancer in 173 (60.5%) and benign conditions in 113 (39.5%). Mean follow-up was 28.8 months; 56 patients died (mean time to death: 26.4 months). Thirteen urologic injuries (4.6%) occurred: 5 urethral, 4 ureteral, 2 bladder, and 2 prostatic. After excluding those with insufficient follow-up, 131 (47.8%) had new or worsening LUTS: 63 (23.0%) incontinence, 85 (30.7%) retention, and 61 (22.3%) with other LUTS (Table 1). Diabetes was associated with increased risk. Of the included 134 men, 34 (25.4%) had new or worsening ED, with 28 (20.9%) requiring treatment.
CONCLUSIONS:Urologic complications following APR are common. A multidisciplinary approach may optimize recovery.
Back to 2025 Abstracts


