Back to 2016 Annual Meeting
Preoperative evaluation protocol for genitourinary vascularized composite allotransplantation
Kai Li, MD, Ilse Schol, BS, Garry Choi, MD, MBA, Tessa Drijkoningen, MD, Raymond W. Liu, MD, Cigdem Tanrikut, MD, Paul Holzer, USNR, Curtis L. Cetrulo, MD, Dicken S. C. Ko, MD, FRCSC.
Massachusetts General Hospital, Boston, MA, USA.
Background:
Genitourinary vascularized composite allotransplantation (GUVCA) potentially represents the next step in improving both urinary and sexual function as well as cosmetic appearance following genitourinary tissue loss. The preoperative evaluation of donors and recipients is multi-modal and multi-disciplinary. Many factors need to be considered including recipient eligibility from a medical and anatomic standpoint as well as appropriate donor selection. To date, the literature that discusses the preoperative considerations of GUVCA is limited. At our institution, we have developed a pre-operative evaluation protocol for potential GUVCA recipients including pre-operative imaging, donor selection, and consultation with multi-disciplinary team. We also describe the critical neurovascular anatomy for allotransplantation with our cadaveric experience
Methods:
We constructed a multidisciplinary GUVCA team composed of transplant surgeon, urologists, plastic surgeons, psychiatrists, transplant coordinators, nurses, social workers, dieticians, and financial coordinators. Evaluation of the recipient begins with education and informed consent. Laboratory testing was obtained including routine CBC, chemistries, LFTs, coagulation panel, blood typing, as well as infectious disease screening and panel reactive antibody for HLA. Routine chest X-ray and EKG are obtained. The patient then undergoes our preoperative imaging protocol: high-resolution computed tomography angiography (CTA), diagnostic angiography, and pelvic and penile magnetic resonance imaging (MRI). From the donor perspective, we worked closely with the New England Organ Bank for recipient listing, donor selection, and donor procurement planning. Using anatomic dissections, we identified the appropriate vascularized pedicles from freshly deceased donor pelvic specimens.
Results
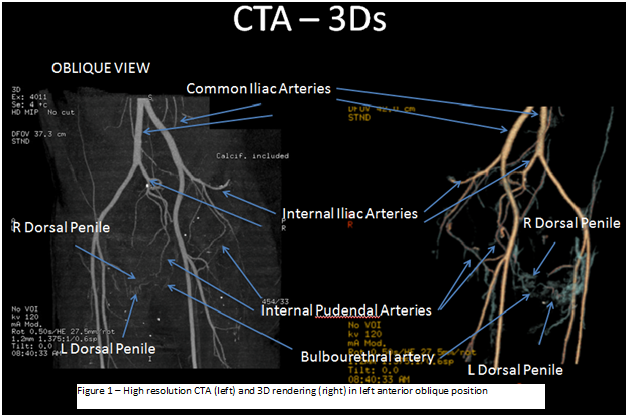
In our pilot experience, we evaluated two potential recipients that underwent the preoperative evaluation protocol. Our imaging protocol assessed for adequacy of recipient anatomy for implantation of the GUVCA graft. Using MRI with high-resolution isometric sequences, we identified neural bundles alongside the internal pudendal artery in the region immediately posterior to the pubic symphysis. MRI with contrast suggested corporal body viability. CTA with volumetric and multiplanar analysis of arterial
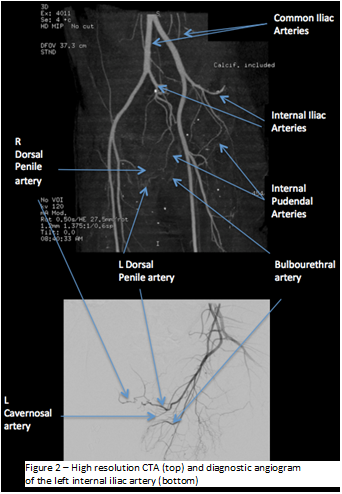
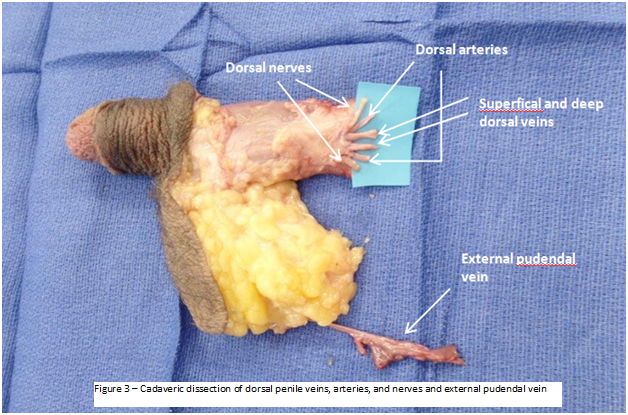
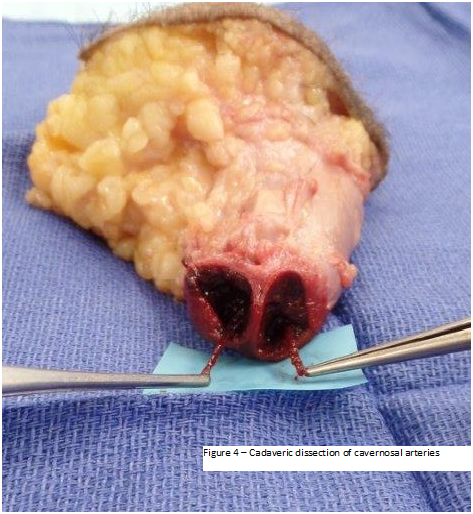
vasculature was critical for assessing vessel adequacy. CTA 3-dimensional rendering was performed for enhanced spatial assessment [figure1]. Diagnostic angiography held advantage over CTA in situations with suboptimal characterization of smaller vessels, e.g. dorsal penile arteries [figure2]. From our dissection experience, we identified all critical nerves and vessels necessary for anastomosis including the superficial and deep dorsal penile veins, dorsal penile arteries, dorsal penile nerves, cavernosal arteries, and external pudendal vessels [figures 3 and 4].
Conclusions
The preoperative protocol presented in this study represents an essential roadmap to surgical planning for GUVCA.
Back to 2016 Annual Meeting
|
|
|
|



