|
Back to 2014 Annual Meeting Abstracts
URETHROLYSIS/SLING TAKE DOWN AFTER ROBOTIC SACROCOLPOPEXY & CONCOMITANT MIDURETHRAL SINTETHIC SLING
Paholo G. Barboglio Romo, MD, MPH1, Veronica Triaca, MD2.
1Dartmouth-Hitchcock, Lebanon, NH, USA, 2Concord Hospital, Concord, NH, USA.
INTRODUCTION/OBJECTIVE: Concomitant mid-urethral synthetic sling (MUSS) at the time of pelvic organ prolapse surgery in women without preoperative stress urinary incontinence reduces the likelihood of occult urinary incontinence after reconstructive surgery but increases the likelihood of adverse events (Wei, N Engl J Med 2012). The aim of our study was to evaluate and analyze those women who required urethrolysis or sling take down after robotic sacrocolpopexy (RS) and concomitant MUSS.
METHODS: IRB approved single surgeon’s retrospective cohort study of women who had RS with concomitant MUSS from April 2010 to October 2012. History and physical exam were performed in all patients and some women underwent urodynamics (UDS) for pre-operative evaluation. Questionnaires were answered in the waiting room area. Follow up was performed at 2 and 6 weeks, then at 3-6 months and one year. Outcomes were analyzed at six months. Sling take down or urethrolysis was performed in those women who developed urinary retention requiring clean intermittent catheterization (CIC). We used PFDI-20 and PFIQ-7 short form questionnaires to evaluate patient subjective data. Pearson’s X2, t-student test, Wilcoxon sum ranks test were used for the analysis.
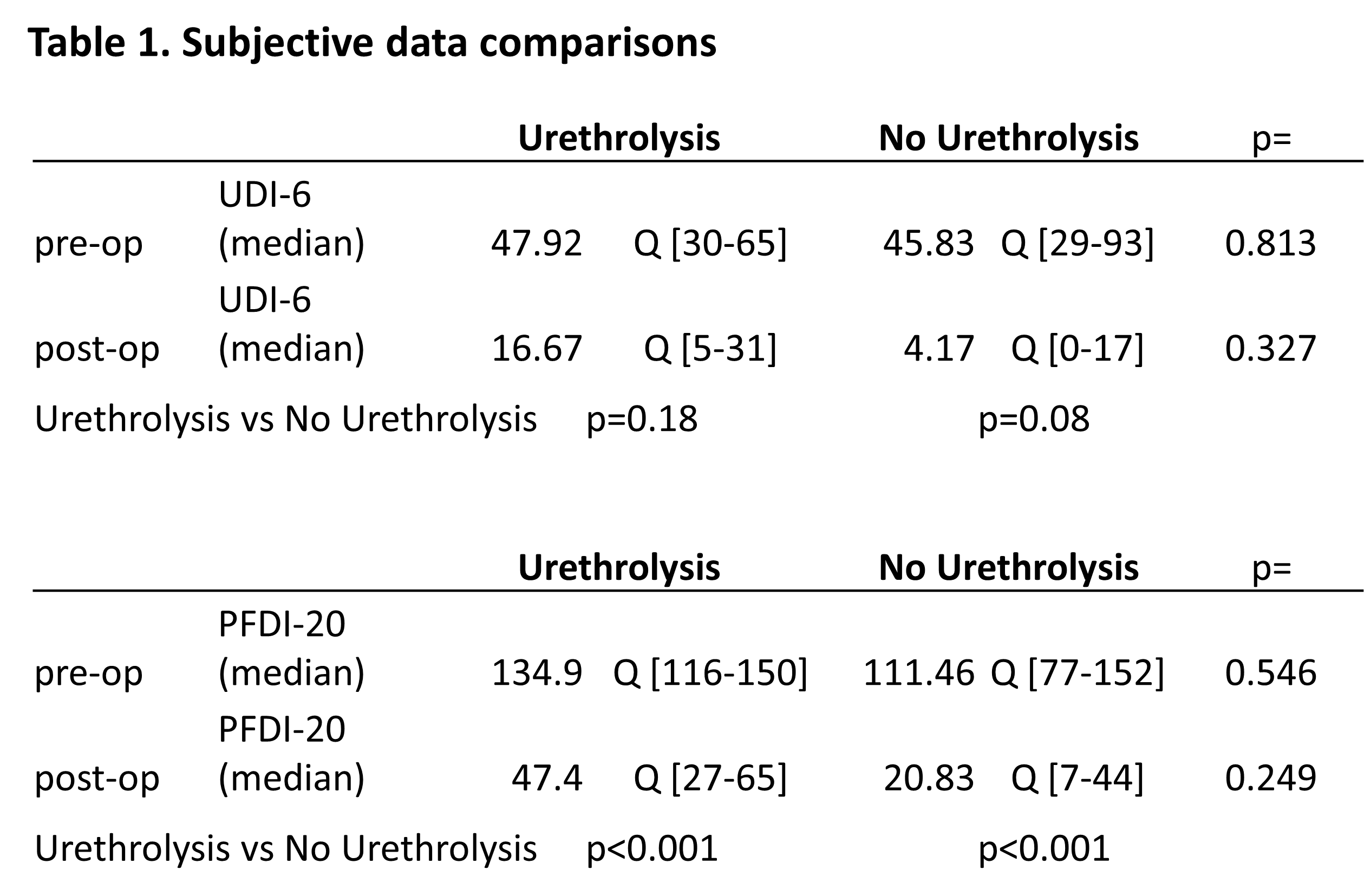
RESULTS: Complete follow up data at six months was available for 140 women. Median age was 59 years old (IQ range [25%-75%] 52-67). Six women (4.2%) developed urinary retention and underwent urethrolysis/sling take down. All of these stopped CIC and four women had at least 70% improvement in either PFDI or PFIQ-7 afterwards. Patients who required sling take down/urethrolysis had lower (p=0.048) body mass index (Median 25.9; IQ[25%-75%] 24.5-26.2) in comparison to the other patients (Median 27.88; IQ[25%-75%] 25.2-32). When assessing pre-operative UDS the only statistical difference was found on first sensation. Women who required sling take down/urethrolysis had lower first sensation volume (X=28.5 SD+/-18.5 vs. X=53.1 SD+/-87.5; p=0.041). Table 1 illustrates subjective outcomes from validated questionnaires. There was no other significant difference when assessing other peri-operative variables including demographics.
CONCLUSION: The rate of post-operative voiding dysfunction and the need for further surgery to address this is low, when placing concomitant MUSS at the time of robotic sacrocolpopexy.
Back to 2014 Annual Meeting Abstracts
|

|
