|
Back to 2014 Annual Meeting Abstracts
Precision of Ureteroscopic Visual Estimation of Stone Fragment Size
Andrew Leone, MD1, Timothy Tran, MD1, Achankeng Afiadata, MS2, Simone Thavaseelan, MD1, Gyan Pareek, MD1, Jennifer Yates, MD2.
1The Warren Alpert Medical School of Brown Univeristy/Kidney Stone Center at Miriam Hospital, Providence, RI, USA, 2UMass Medical Center, Worcester, MA, USA.
Background: We sought to establish the accuracy of fellowship trained endurologists in estimating in vivo stone fragment size during flexible ureterorenoscopy by comparing visual estimated size to measured size. Previously other literature has investigated endourologists accuracy at predicting ex vivo stone fragment size.
Methods: An IRB approved prospective study was conducted with all patients undergoing laser lithotripsy for renal and ureteral stones by three fellowship trained endurologists from November 2013 to February 2014. In all patients ureteral access sheaths were successfully placed and there was no deviation from standard management of surgeons’ clinical practice. The size of 61 stone fragments in 15 patients was initially visually estimated by the surgeon from estimation based on the size of the laser fiber (in all cases a 200 micron laser fiber) and a 0 tip nitinol basket (all cases 1.9 Fr) . The stone fragment was then basket extracted using a standard 0 tip nitinol stone basket and the largest dimension of the stone was measured by the surgeon using a ruler. Accuracy of measurement was performed by creation of correlation coefficients and creation of Altman-Brand plots.
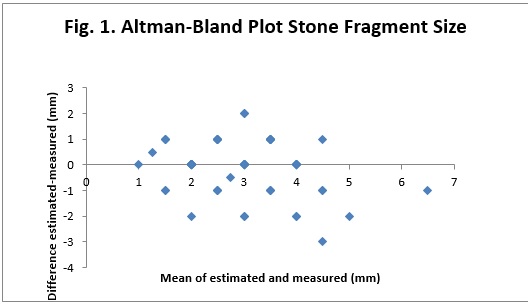
Results: Fellowship trained endourologists overall underestimated stone size by 0.11 mm. The correlation coefficient was r=0.61 with p value <0.00001. Stones smaller than 4mm were overestimated by 0.25 mm (R=0.49, p=<0.0001) and stones larger than 4 mm were underestimated by 0.94 mm (R=0.39, P=0.09). Altman-Brand plots demonstrated that the endourologists estimated stone size within a range of -0.11 to 1.42 mm (Figure 1). There were no complications encountered in any of the patients.
Conclusion: Endourologists overall underestimated stone fragment size during ureterorenoscopy. However when subdivided based upon stone fragment size, stone fragments smaller than 4 mm were overestimated and those larger than 4 mm were underestimated. Further research is needed to determine if technology or surgeon training can improve measurement accuracy of in vivo stone fragments. Future research will look at improvement over time with repeated estimations and if varying the size of laser fiber/basket utilized can improve precision. Because of slight underestimation of fragment size we recommend performing basket stone extraction at the conclusion of ureterorenoscopy as a final check in order to improve stone fee rates.
Back to 2014 Annual Meeting Abstracts
|

|
