|
Back to 2014 Annual Meeting Abstracts
The Efficacy of Congenital Penile Curvature Repair in Pre-Adolescent Males without Hypospadias: Early Outcomes
Joseph W. McQuaid, MD1, Emilie K. Johnson, MD, MPH2, Elizabeth West, BS2, Ilina Rosoklija, MPH2, Marc Cendron, MD2.
1Massachusetts General Hospital, Cambridge, MA, USA, 2Boston Children's Hospital, Boston, MA, USA.
INTRODUCTION:
Congenital penile curvature (CPC, or so-called chordee) most frequently occurs in tandem with hypospadias, however in rare cases it may be seen with an orthotopic urethral meatus. CPC without hypospadias presents in a variety of forms including curvature isolated to a single plane or multi-planar angulation. Our objective was to review our surgical experience and outcomes for patients with CPC.
MATERIALS AND METHODS:
We performed a retrospective study of boys with CPC who underwent penile straightening between 2008 and 2010 at our institution. Patients with hypospadias, epispadias, bladder exstrophy, or prior penile reconstruction were excluded. Records were reviewed for Donnahoo classification, surgical indication and technique, and post-operative outcomes including complications, recurrent curvature, and urinary complaints.
RESULTS:
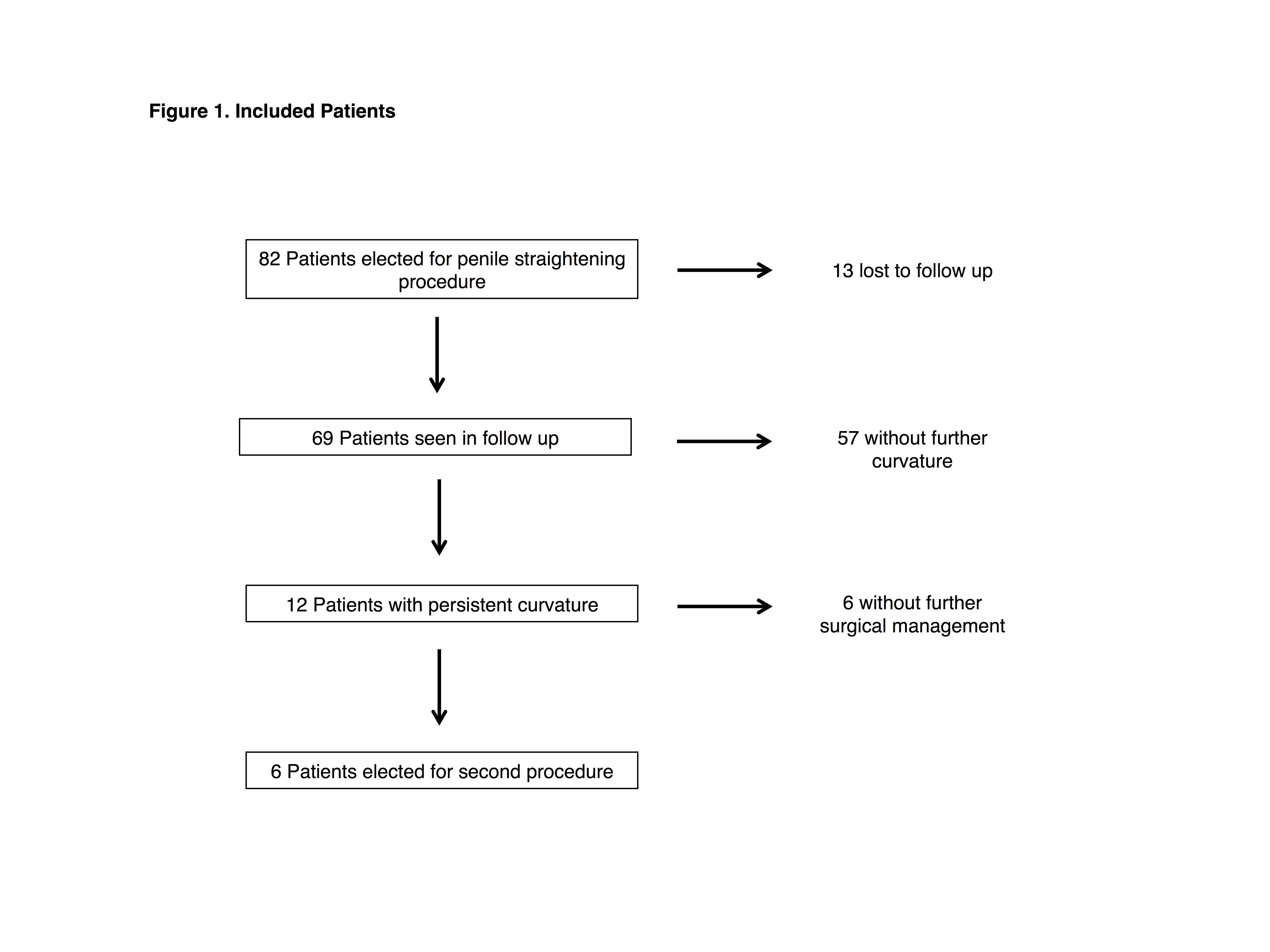
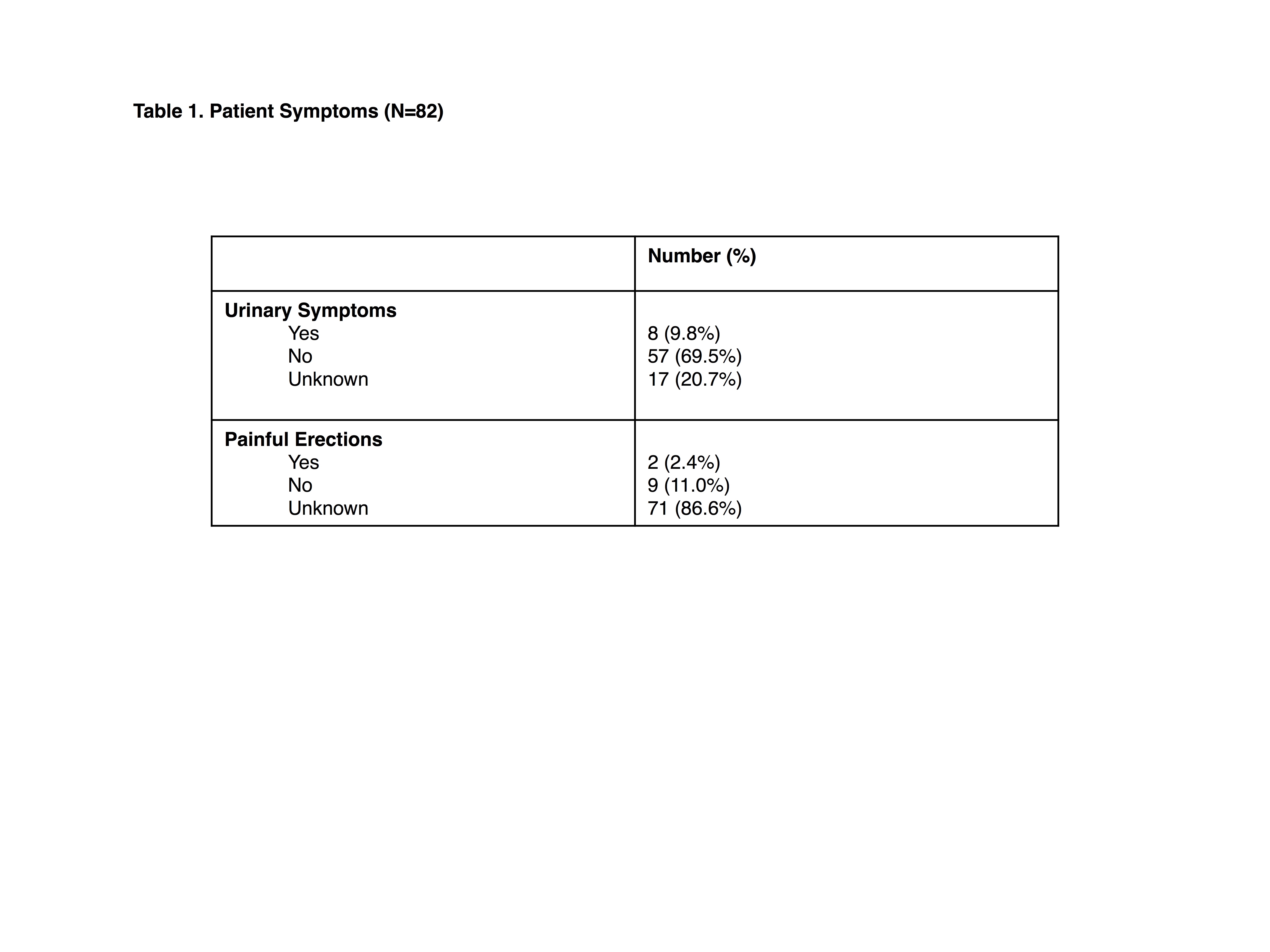
We identified 82 patients (mean age 1.7 years) who had CPC without hypospadias and underwent penile straightening (Figure 1). The most common anatomic variants were ventral (37%) and multi-planar (34%) angulation, with dorsal (13%) and lateral (16%) curvature being less common. Although 75% demonstrated >30° curvature, few children were symptomatic (Table 1). Reported symptoms included painful erections (2 patients) and urinary complaints (8 patients). Curved stream was noted in 77% and urinary spray in 13% of these cases. Multiple surgical techniques were used in combination including tunical plications (39%), excision of fibrotic tissue (30%), and use of the Nesbit (4%) and modified Nesbit techniques (11%); 45% had an artificial erection test recorded as part of their procedure. However, the most common approach (35/82, 42.7%) was degloving and reapproximating the penile skin alone. This was mirrored in patients' Donnahoo classification: 42% skin chordee, 33% dysgenetic Buck’s/dartos fasciae, and 14% corporal disproportion. Complication occurred in 9% of patients including wound separation, hematoma, and skin infection requiring oral antibitoics. Twelve boys (17%) showed persistent curvature, but the degree was milder than preop (33% had curvature >30°). All 6 who underwent a 2nd procedure had either dysgenetic fasciae or corporal disproportion.
CONCLUSIONS:
Our data suggest that CPC without hypospadias most often presents with significant (>30°) penile angulation and yet is frequently due to skin chordee alone. However, one procedure is not adequate for all patients, and dysgenetic fasciae and corporal disproportion appear to be more frequent in patients requiring reoperation. More stringent use of the artificial erection test may facilitate identification of patients requiring aggressive management during their initial procedure including excision of fibrotic tissue and/or plication-based techniques.
Back to 2014 Annual Meeting Abstracts
|

|
